 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeLeMAJ (Legal LLM-as-a-Judge): Bridging Legal Reasoning and LLM Evaluation
Oct 08, 2025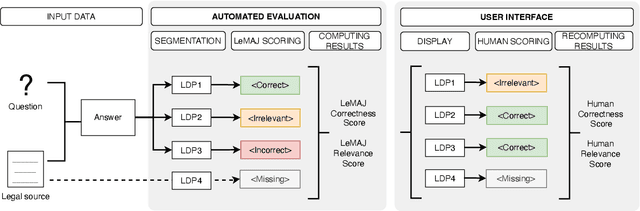
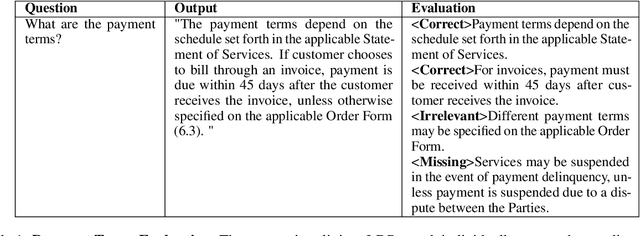
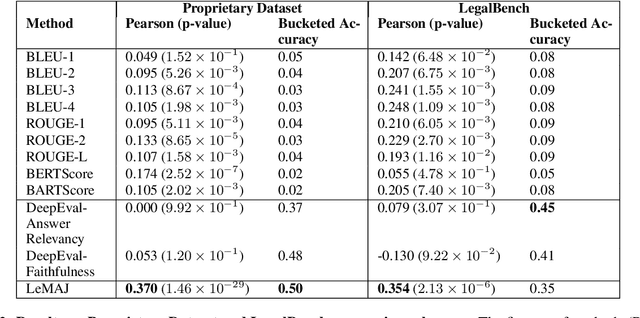
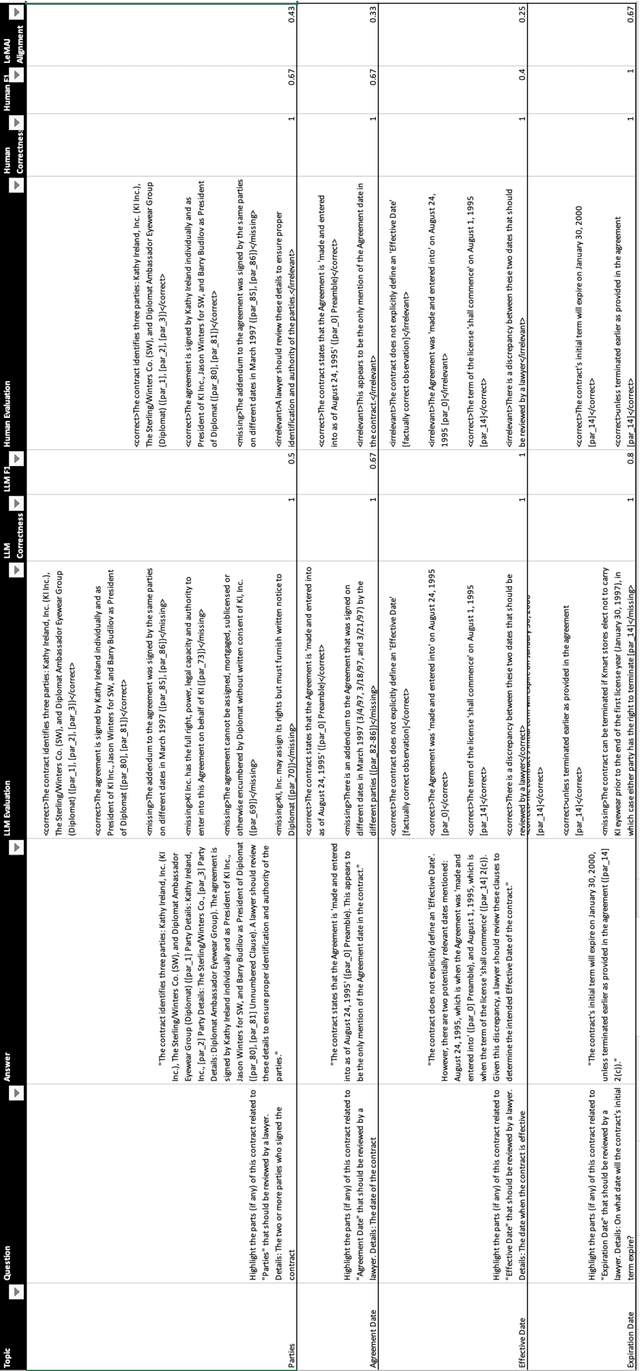
Evaluating large language model (LLM) outputs in the legal domain presents unique challenges due to the complex and nuanced nature of legal analysis. Current evaluation approaches either depend on reference data, which is costly to produce, or use standardized assessment methods, both of which have significant limitations for legal applications. Although LLM-as-a-Judge has emerged as a promising evaluation technique, its reliability and effectiveness in legal contexts depend heavily on evaluation processes unique to the legal industry and how trustworthy the evaluation appears to the human legal expert. This is where existing evaluation methods currently fail and exhibit considerable variability. This paper aims to close the gap: a) we break down lengthy responses into 'Legal Data Points' (LDPs), self-contained units of information, and introduce a novel, reference-free evaluation methodology that reflects how lawyers evaluate legal answers; b) we demonstrate that our method outperforms a variety of baselines on both our proprietary dataset and an open-source dataset (LegalBench); c) we show how our method correlates more closely with human expert evaluations and helps improve inter-annotator agreement; and finally d) we open source our Legal Data Points for a subset of LegalBench used in our experiments, allowing the research community to replicate our results and advance research in this vital area of LLM evaluation on legal question-answering.
Gemini 1.5: Unlocking multimodal understanding across millions of tokens of context
Mar 08, 2024In this report, we present the latest model of the Gemini family, Gemini 1.5 Pro, a highly compute-efficient multimodal mixture-of-experts model capable of recalling and reasoning over fine-grained information from millions of tokens of context, including multiple long documents and hours of video and audio. Gemini 1.5 Pro achieves near-perfect recall on long-context retrieval tasks across modalities, improves the state-of-the-art in long-document QA, long-video QA and long-context ASR, and matches or surpasses Gemini 1.0 Ultra's state-of-the-art performance across a broad set of benchmarks. Studying the limits of Gemini 1.5 Pro's long-context ability, we find continued improvement in next-token prediction and near-perfect retrieval (>99%) up to at least 10M tokens, a generational leap over existing models such as Claude 2.1 (200k) and GPT-4 Turbo (128k). Finally, we highlight surprising new capabilities of large language models at the frontier; when given a grammar manual for Kalamang, a language with fewer than 200 speakers worldwide, the model learns to translate English to Kalamang at a similar level to a person who learned from the same content.
Gemini: A Family of Highly Capable Multimodal Models
Dec 19, 2023This report introduces a new family of multimodal models, Gemini, that exhibit remarkable capabilities across image, audio, video, and text understanding. The Gemini family consists of Ultra, Pro, and Nano sizes, suitable for applications ranging from complex reasoning tasks to on-device memory-constrained use-cases. Evaluation on a broad range of benchmarks shows that our most-capable Gemini Ultra model advances the state of the art in 30 of 32 of these benchmarks - notably being the first model to achieve human-expert performance on the well-studied exam benchmark MMLU, and improving the state of the art in every one of the 20 multimodal benchmarks we examined. We believe that the new capabilities of Gemini models in cross-modal reasoning and language understanding will enable a wide variety of use cases and we discuss our approach toward deploying them responsibly to users.
Batch Calibration: Rethinking Calibration for In-Context Learning and Prompt Engineering
Sep 29, 2023



Prompting and in-context learning (ICL) have become efficient learning paradigms for large language models (LLMs). However, LLMs suffer from prompt brittleness and various bias factors in the prompt, including but not limited to the formatting, the choice verbalizers, and the ICL examples. To address this problem that results in unexpected performance degradation, calibration methods have been developed to mitigate the effects of these biases while recovering LLM performance. In this work, we first conduct a systematic analysis of the existing calibration methods, where we both provide a unified view and reveal the failure cases. Inspired by these analyses, we propose Batch Calibration (BC), a simple yet intuitive method that controls the contextual bias from the batched input, unifies various prior approaches, and effectively addresses the aforementioned issues. BC is zero-shot, inference-only, and incurs negligible additional costs. In the few-shot setup, we further extend BC to allow it to learn the contextual bias from labeled data. We validate the effectiveness of BC with PaLM 2-(S, M, L) and CLIP models and demonstrate state-of-the-art performance over previous calibration baselines across more than 10 natural language understanding and image classification tasks.
STUDY: Socially Aware Temporally Casual Decoder Recommender Systems
Jun 02, 2023With the overwhelming amount of data available both on and offline today, recommender systems have become much needed to help users find items tailored to their interests. When social network information exists there are methods that utilize this information to make better recommendations, however the methods are often clunky with complex architectures and training procedures. Furthermore many of the existing methods utilize graph neural networks which are notoriously difficult to train. To address this, we propose Socially-aware Temporally caUsal Decoder recommender sYstems (STUDY). STUDY does joint inference over groups of users who are adjacent in the social network graph using a single forward pass of a modified transformer decoder network. We test our method in a school-based educational content setting, using classroom structure to define social networks. Our method outperforms both social and sequential methods while maintaining the design simplicity of a single homogeneous network that models all interactions in the data. We also carry out ablation studies to understand the drivers of our performance gains and find that our model depends on leveraging a social network structure that effectively models the similarities in user behavior.
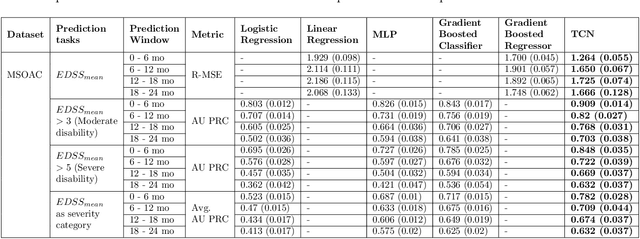
Longitudinal Modeling of Multiple Sclerosis using Continuous Time Models
Feb 15, 2023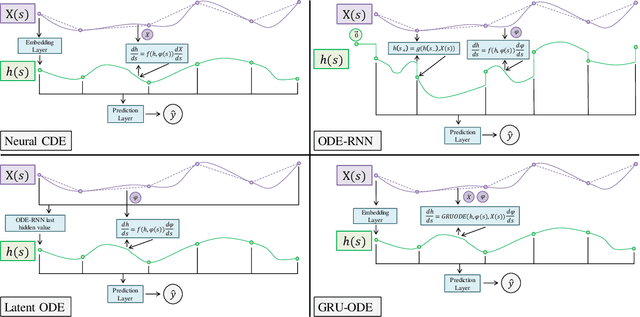
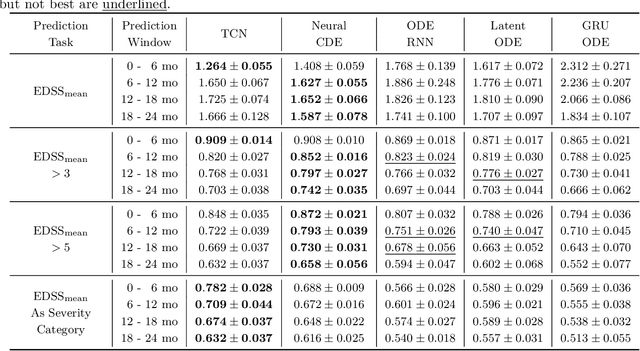
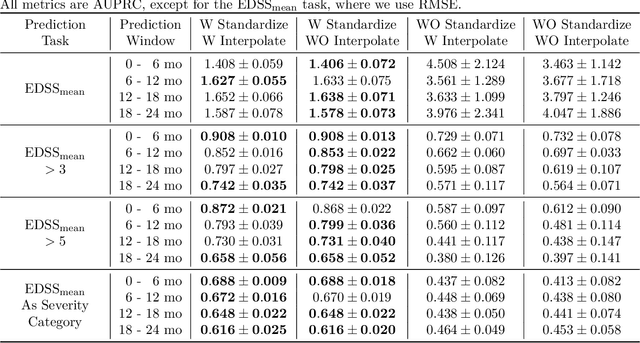
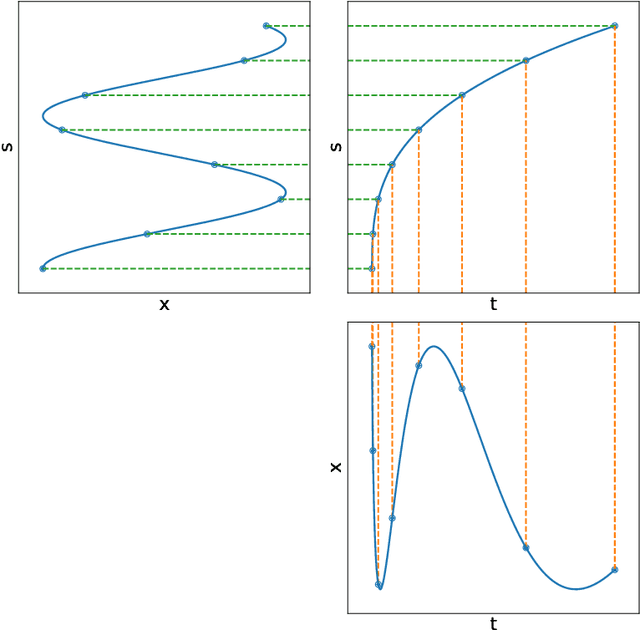
Multiple sclerosis is a disease that affects the brain and spinal cord, it can lead to severe disability and has no known cure. The majority of prior work in machine learning for multiple sclerosis has been centered around using Magnetic Resonance Imaging scans or laboratory tests; these modalities are both expensive to acquire and can be unreliable. In a recent paper it was shown that disease progression can be predicted effectively using performance outcome measures (POMs) and demographic data. In our work we extend on this to focus on the modeling side, using continuous time models on POMs and demographic data to predict progression. We evaluate four continuous time models using a publicly available multiple sclerosis dataset. We find that continuous models are often able to outperform discrete time models. We also carry out an extensive ablation to discover the sources of performance gains, we find that standardizing existing features leads to a larger performance increase than interpolating missing features.
Disability prediction in multiple sclerosis using performance outcome measures and demographic data
Apr 08, 2022


Literature on machine learning for multiple sclerosis has primarily focused on the use of neuroimaging data such as magnetic resonance imaging and clinical laboratory tests for disease identification. However, studies have shown that these modalities are not consistent with disease activity such as symptoms or disease progression. Furthermore, the cost of collecting data from these modalities is high, leading to scarce evaluations. In this work, we used multi-dimensional, affordable, physical and smartphone-based performance outcome measures (POM) in conjunction with demographic data to predict multiple sclerosis disease progression. We performed a rigorous benchmarking exercise on two datasets and present results across 13 clinically actionable prediction endpoints and 6 machine learning models. To the best of our knowledge, our results are the first to show that it is possible to predict disease progression using POMs and demographic data in the context of both clinical trials and smartphone-base studies by using two datasets. Moreover, we investigate our models to understand the impact of different POMs and demographics on model performance through feature ablation studies. We also show that model performance is similar across different demographic subgroups (based on age and sex). To enable this work, we developed an end-to-end reusable pre-processing and machine learning framework which allows quicker experimentation over disparate MS datasets.
Healthsheet: Development of a Transparency Artifact for Health Datasets
Feb 26, 2022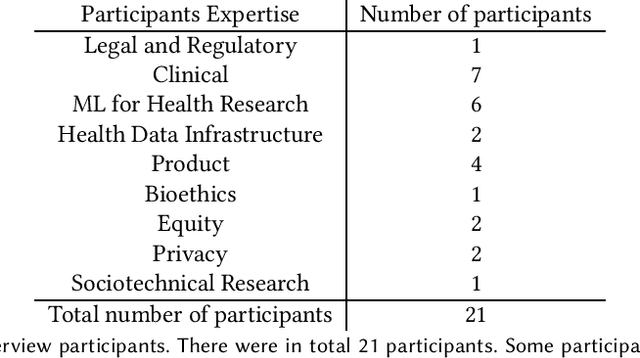
Machine learning (ML) approaches have demonstrated promising results in a wide range of healthcare applications. Data plays a crucial role in developing ML-based healthcare systems that directly affect people's lives. Many of the ethical issues surrounding the use of ML in healthcare stem from structural inequalities underlying the way we collect, use, and handle data. Developing guidelines to improve documentation practices regarding the creation, use, and maintenance of ML healthcare datasets is therefore of critical importance. In this work, we introduce Healthsheet, a contextualized adaptation of the original datasheet questionnaire ~\cite{gebru2018datasheets} for health-specific applications. Through a series of semi-structured interviews, we adapt the datasheets for healthcare data documentation. As part of the Healthsheet development process and to understand the obstacles researchers face in creating datasheets, we worked with three publicly-available healthcare datasets as our case studies, each with different types of structured data: Electronic health Records (EHR), clinical trial study data, and smartphone-based performance outcome measures. Our findings from the interviewee study and case studies show 1) that datasheets should be contextualized for healthcare, 2) that despite incentives to adopt accountability practices such as datasheets, there is a lack of consistency in the broader use of these practices 3) how the ML for health community views datasheets and particularly \textit{Healthsheets} as diagnostic tool to surface the limitations and strength of datasets and 4) the relative importance of different fields in the datasheet to healthcare concerns.
Maintaining fairness across distribution shift: do we have viable solutions for real-world applications?
Feb 02, 2022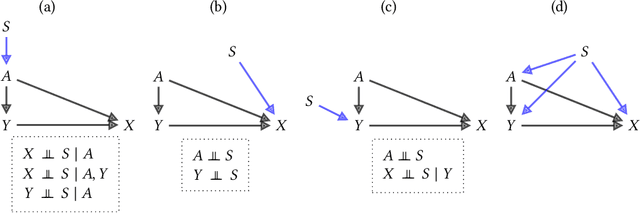
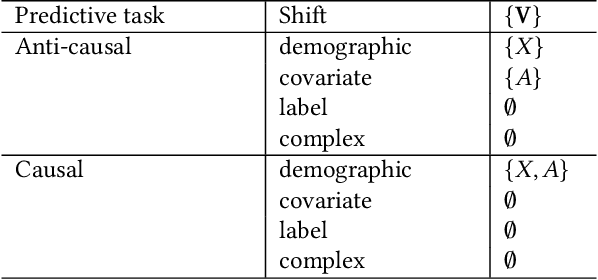
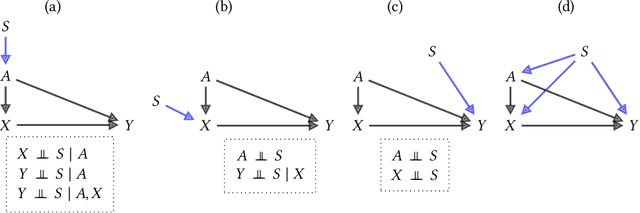
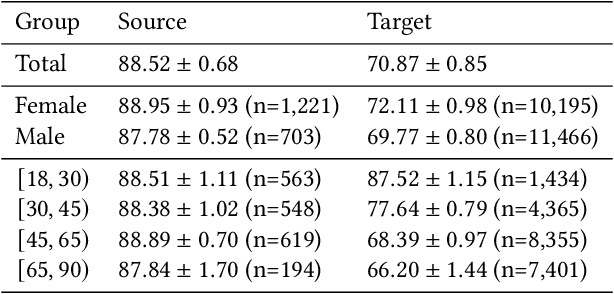
Fairness and robustness are often considered as orthogonal dimensions when evaluating machine learning models. However, recent work has revealed interactions between fairness and robustness, showing that fairness properties are not necessarily maintained under distribution shift. In healthcare settings, this can result in e.g. a model that performs fairly according to a selected metric in "hospital A" showing unfairness when deployed in "hospital B". While a nascent field has emerged to develop provable fair and robust models, it typically relies on strong assumptions about the shift, limiting its impact for real-world applications. In this work, we explore the settings in which recently proposed mitigation strategies are applicable by referring to a causal framing. Using examples of predictive models in dermatology and electronic health records, we show that real-world applications are complex and often invalidate the assumptions of such methods. Our work hence highlights technical, practical, and engineering gaps that prevent the development of robustly fair machine learning models for real-world applications. Finally, we discuss potential remedies at each step of the machine learning pipeline.
Best of both worlds: local and global explanations with human-understandable concepts
Jun 16, 2021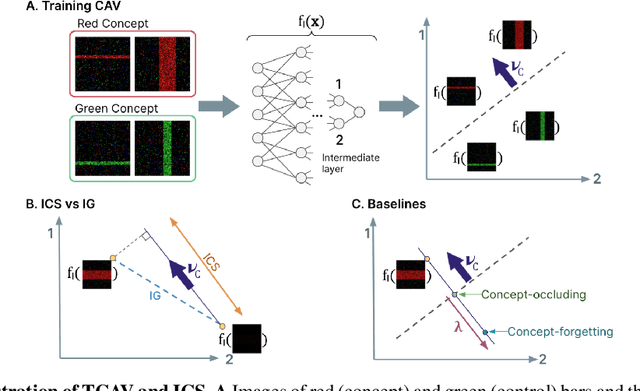
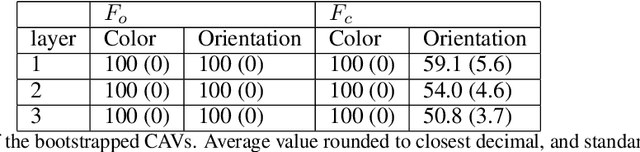
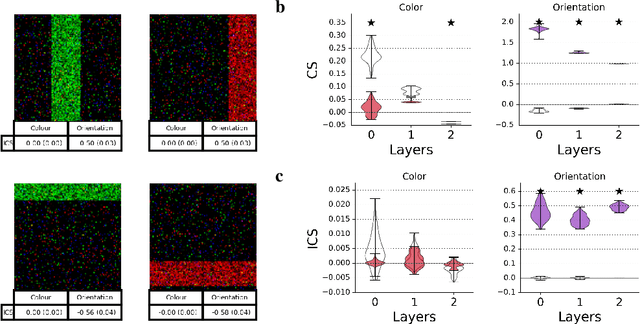
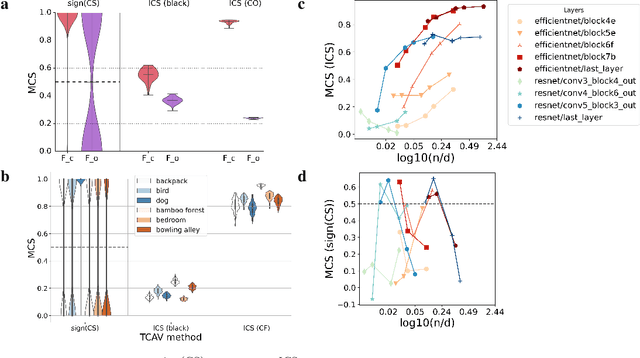
Interpretability techniques aim to provide the rationale behind a model's decision, typically by explaining either an individual prediction (local explanation, e.g. `why is this patient diagnosed with this condition') or a class of predictions (global explanation, e.g. `why are patients diagnosed with this condition in general'). While there are many methods focused on either one, few frameworks can provide both local and global explanations in a consistent manner. In this work, we combine two powerful existing techniques, one local (Integrated Gradients, IG) and one global (Testing with Concept Activation Vectors), to provide local, and global concept-based explanations. We first validate our idea using two synthetic datasets with a known ground truth, and further demonstrate with a benchmark natural image dataset. We test our method with various concepts, target classes, model architectures and IG baselines. We show that our method improves global explanations over TCAV when compared to ground truth, and provides useful insights. We hope our work provides a step towards building bridges between many existing local and global methods to get the best of both worlds.