 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeEvaluation of Augmented Reality-based Intuitive Interface for Robot-Assisted Transesophageal Echocardiography: A User Study
Jun 18, 2026TransEsophageal Echocardiography (TEE) is essential for diagnosing and guiding Structural Heart Disease (SHD) interventions. However, manual TEE manipulation demands significant operator expertise, is physically demanding, and exposes clinicians to radiation when performed alongside fluoroscopy. Robotic-assisted TEE systems have been introduced to improve probe handling and reduce operator fatigue, yet the design of intuitive and effective user interfaces remains an open challenge. This study presents and evaluates a model-enhanced, Augmented Reality (AR)-based intuitive interface for robot-assisted TEE, designed to improve spatial awareness and control intuitiveness. A robotic TEE platform integrated with electromagnetic tracking and a virtual simulator was used to compare three user interfaces differing in visualization and interaction modalities: 2D jointlevel (2D-JI), 3D joint-level (3D-JI), and 3D tip-level (3D-TI). Thirty six participants performed standardized navigation tasks to reproduce target echocardiographic views, with performance assessed via position and orientation errors, completion time, and NASA-TLX workload scores. Results show that 3D visualization significantly improved spatial accuracy, reducing median position error from 13 mm to 3 mm and halving the orientation error compared with the 2D interface. Tip-level interaction yielded a further 50% reduction in orientation error and reduced interuser variability relative to joint-level control. Overall, the 3D-TI configuration, combining immersive visualization with direct tip-level control, proved the most effective and ergonomic interface, supporting the integration of AR-based visualization and intuitive control paradigms into next-generation robotic TEE systems to enhance operator performance and procedural safety.
Standardisation of Convex Ultrasound Data Through Geometric Analysis and Augmentation
Feb 13, 2025



The application of ultrasound in healthcare has seen increased diversity and importance. Unlike other medical imaging modalities, ultrasound research and development has historically lagged, particularly in the case of applications with data-driven algorithms. A significant issue with ultrasound is the extreme variability of the images, due to the number of different machines available and the possible combination of parameter settings. One outcome of this is the lack of standardised and benchmarking ultrasound datasets. The method proposed in this article is an approach to alleviating this issue of disorganisation. For this purpose, the issue of ultrasound data sparsity is examined and a novel perspective, approach, and solution is proposed; involving the extraction of the underlying ultrasound plane within the image and representing it using annulus sector geometry. An application of this methodology is proposed, which is the extraction of scan lines and the linearisation of convex planes. Validation of the robustness of the proposed method is performed on both private and public data. The impact of deformation and the invertibility of augmentation using the estimated annulus sector parameters is also studied. Keywords: Ultrasound, Annulus Sector, Augmentation, Linearisation.
S2C2A: A Flexible Task Space Planning and Control Strategy for Modular Soft Robot Arms
Oct 04, 2024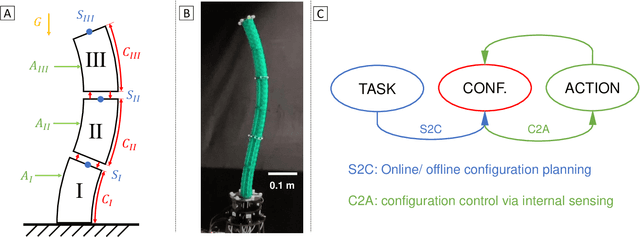
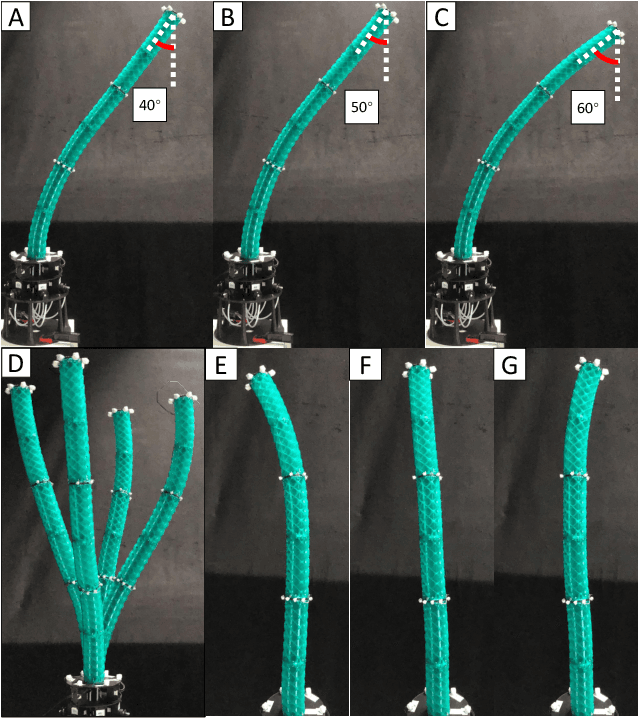
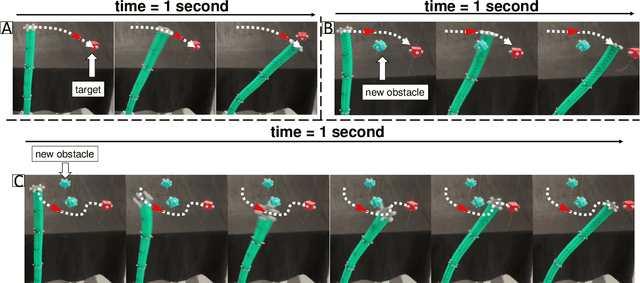
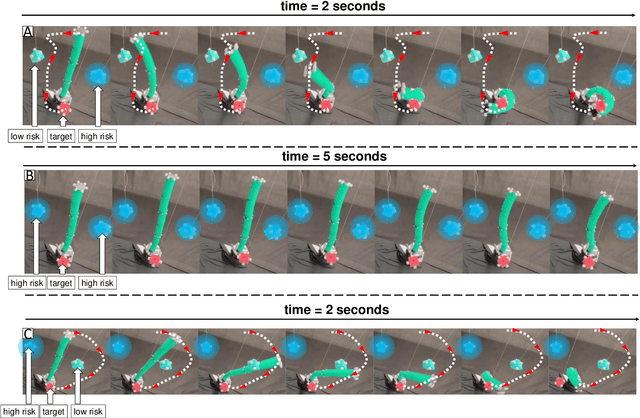
Modular soft robot arms (MSRAs) are composed of multiple independent modules connected in a sequence. Due to their modular structure and high degrees of freedom (DOFs), these modules can simultaneously bend at different angles in various directions, enabling complex deformation. This capability allows MSRAs to perform more intricate tasks than single module robots. However, the modular structure also induces challenges in accurate planning, modeling, and control. Nonlinearity, hysteresis, and gravity complicate the physical model, while the modular structure and increased DOFs further lead to accumulative errors along the sequence. To address these challenges, we propose a flexible task space planning and control strategy for MSRAs, named S2C2A (State to Configuration to Action). Our approach formulates an optimization problem, S2C (State to Configuration planning), which integrates various loss functions and a forward MSRA model to generate configuration trajectories based on target MSRA states. Given the model complexity, we leverage a biLSTM network as the forward model. Subsequently, a configuration controller C2A (Configuration to Action control) is implemented to follow the planned configuration trajectories, leveraging only inaccurate internal sensing feedback. Both a biLSTM network and a physical model are utilized for configuration control. We validated our strategy using a cable-driven MSRA, demonstrating its ability to perform diverse offline tasks such as position control, orientation control, and obstacle avoidance. Furthermore, our strategy endows MSRA with online interaction capability with targets and obstacles. Future work will focus on addressing MSRA challenges, such as developing more accurate physical models and reducing configuration estimation errors along the module sequence.
Autonomous Navigation for Robot-assisted Intraluminal and Endovascular Procedures: A Systematic Review
May 06, 2023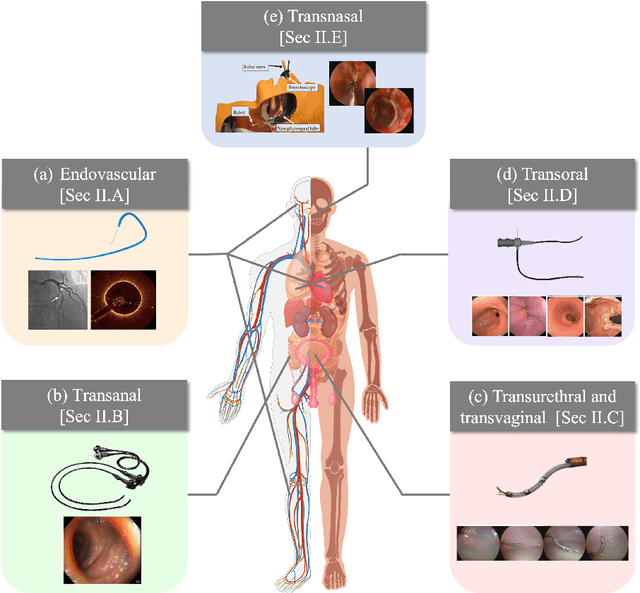
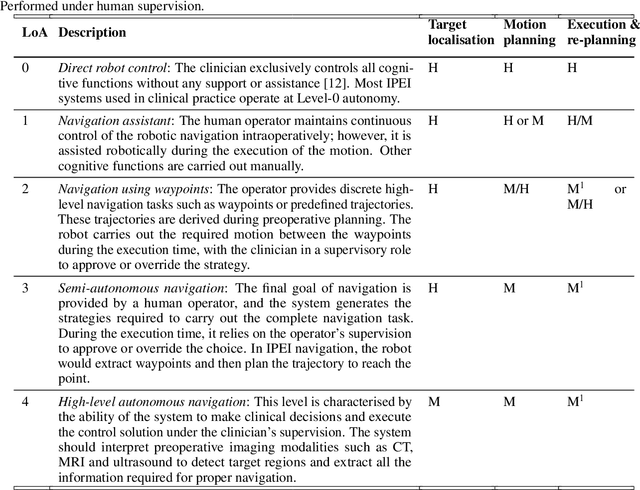
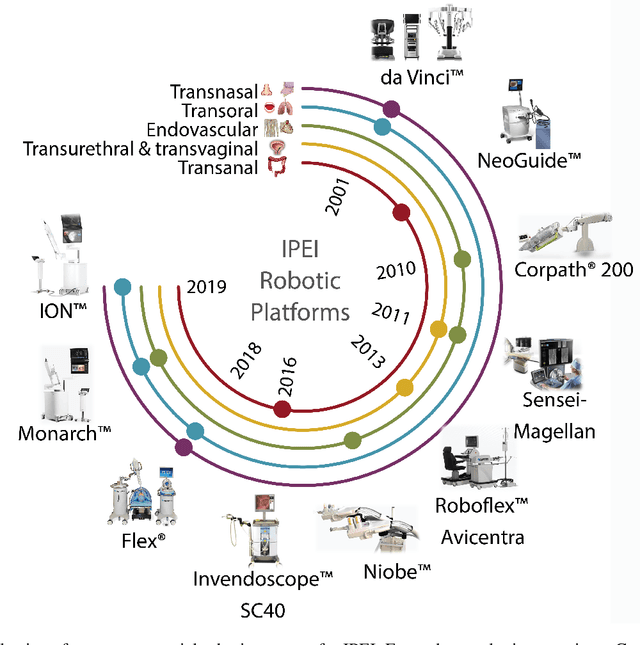
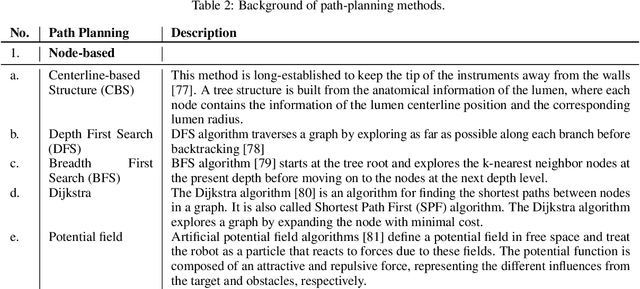
Increased demand for less invasive procedures has accelerated the adoption of Intraluminal Procedures (IP) and Endovascular Interventions (EI) performed through body lumens and vessels. As navigation through lumens and vessels is quite complex, interest grows to establish autonomous navigation techniques for IP and EI for reaching the target area. Current research efforts are directed toward increasing the Level of Autonomy (LoA) during the navigation phase. One key ingredient for autonomous navigation is Motion Planning (MP) techniques. This paper provides an overview of MP techniques categorizing them based on LoA. Our analysis investigates advances for the different clinical scenarios. Through a systematic literature analysis using the PRISMA method, the study summarizes relevant works and investigates the clinical aim, LoA, adopted MP techniques, and validation types. We identify the limitations of the corresponding MP methods and provide directions to improve the robustness of the algorithms in dynamic intraluminal environments. MP for IP and EI can be classified into four subgroups: node, sampling, optimization, and learning-based techniques, with a notable rise in learning-based approaches in recent years. One of the review's contributions is the identification of the limiting factors in IP and EI robotic systems hindering higher levels of autonomous navigation. In the future, navigation is bound to become more autonomous, placing the clinician in a supervisory position to improve control precision and reduce workload.
Uncertainty-aware Self-supervised Learning for Cross-domain Technical Skill Assessment in Robot-assisted Surgery
Apr 28, 2023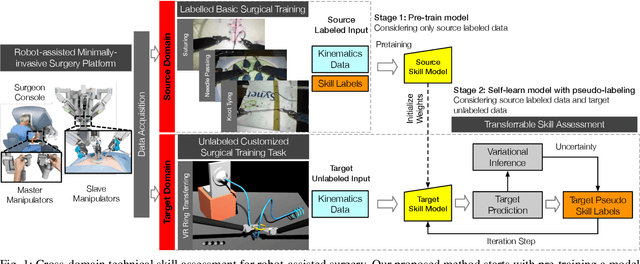
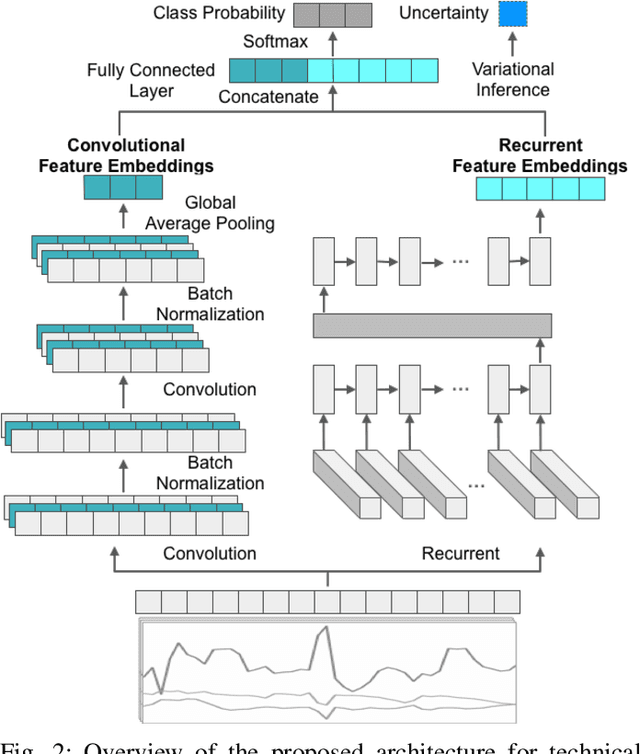
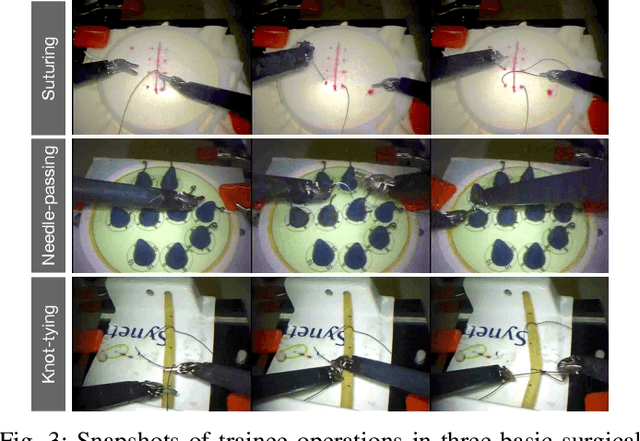
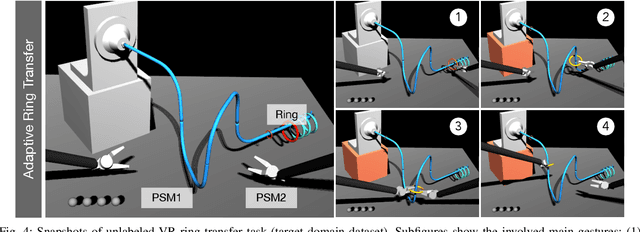
Objective technical skill assessment is crucial for effective training of new surgeons in robot-assisted surgery. With advancements in surgical training programs in both physical and virtual environments, it is imperative to develop generalizable methods for automatically assessing skills. In this paper, we propose a novel approach for skill assessment by transferring domain knowledge from labeled kinematic data to unlabeled data. Our approach leverages labeled data from common surgical training tasks such as Suturing, Needle Passing, and Knot Tying to jointly train a model with both labeled and unlabeled data. Pseudo labels are generated for the unlabeled data through an iterative manner that incorporates uncertainty estimation to ensure accurate labeling. We evaluate our method on a virtual reality simulated training task (Ring Transfer) using data from the da Vinci Research Kit (dVRK). The results show that trainees with robotic assistance have significantly higher expert probability compared to these without any assistance, p < 0.05, which aligns with previous studies showing the benefits of robotic assistance in improving training proficiency. Our method offers a significant advantage over other existing works as it does not require manual labeling or prior knowledge of the surgical training task for robot-assisted surgery.
Colonoscopy Navigation using End-to-End Deep Visuomotor Control: A User Study
Jun 30, 2022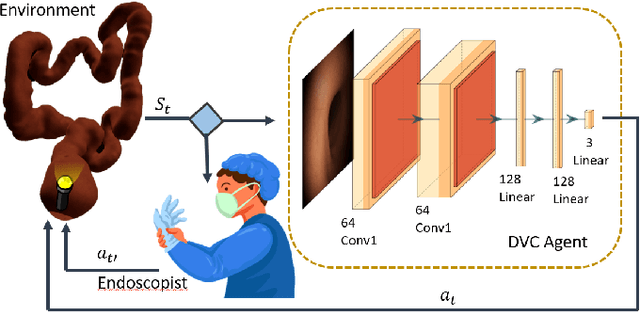
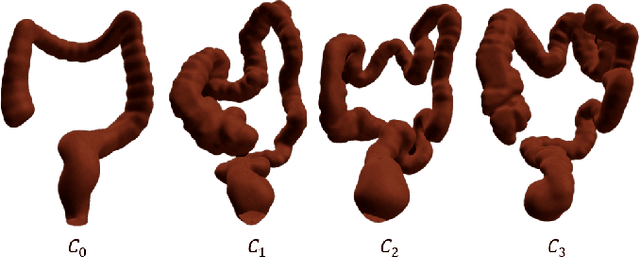
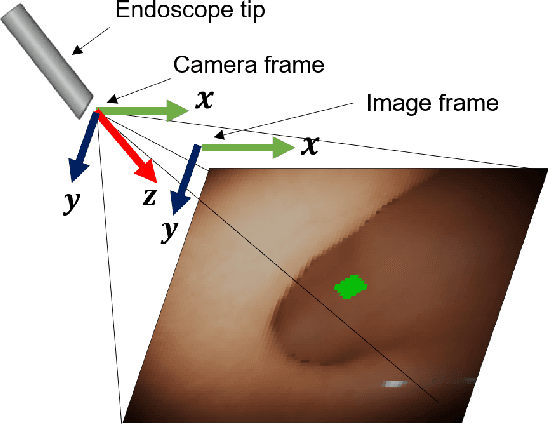
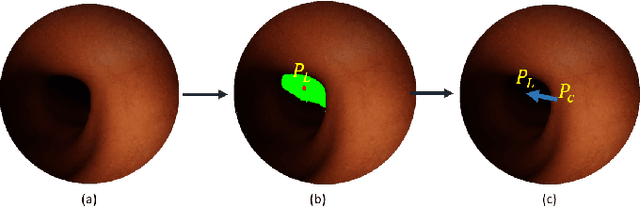
Flexible endoscopes for colonoscopy present several limitations due to their inherent complexity, resulting in patient discomfort and lack of intuitiveness for clinicians. Robotic devices together with autonomous control represent a viable solution to reduce the workload of endoscopists and the training time while improving the overall procedure outcome. Prior works on autonomous endoscope control use heuristic policies that limit their generalisation to the unstructured and highly deformable colon environment and require frequent human intervention. This work proposes an image-based control of the endoscope using Deep Reinforcement Learning, called Deep Visuomotor Control (DVC), to exhibit adaptive behaviour in convoluted sections of the colon tract. DVC learns a mapping between the endoscopic images and the control signal of the endoscope. A first user study of 20 expert gastrointestinal endoscopists was carried out to compare their navigation performance with DVC policies using a realistic virtual simulator. The results indicate that DVC shows equivalent performance on several assessment parameters, being more safer. Moreover, a second user study with 20 novice participants was performed to demonstrate easier human supervision compared to a state-of-the-art heuristic control policy. Seamless supervision of colonoscopy procedures would enable interventionists to focus on the medical decision rather than on the control problem of the endoscope.
Accelerating Surgical Robotics Research: Reviewing 10 Years of Research with the dVRK
May 13, 2021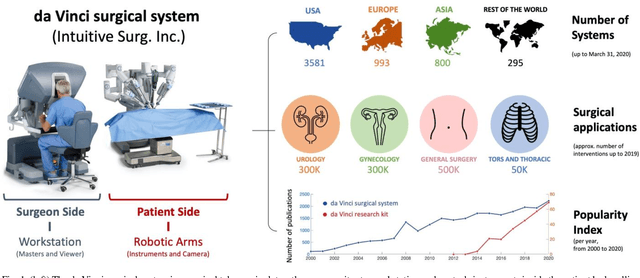
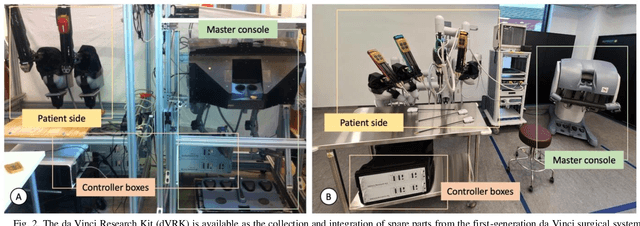
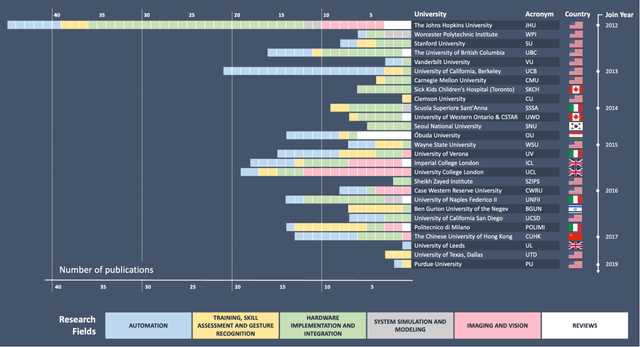
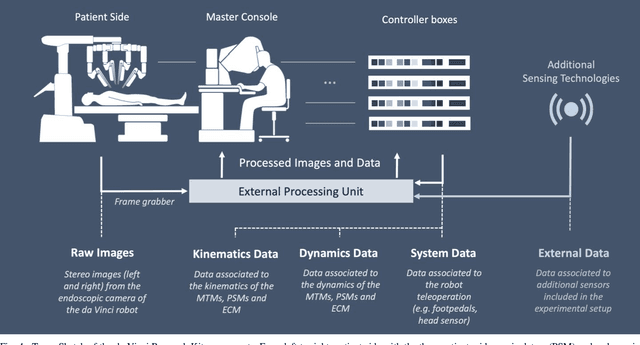
Robotic-assisted surgery is now well-established in clinical practice and has become the gold standard clinical treatment option for several clinical indications. The field of robotic-assisted surgery is expected to grow substantially in the next decade with a range of new robotic devices emerging to address unmet clinical needs across different specialities. A vibrant surgical robotics research community is pivotal for conceptualizing such new systems as well as for developing and training the engineers and scientists to translate them into practice. The da Vinci Research Kit (dVRK), an academic and industry collaborative effort to re-purpose decommissioned da Vinci surgical systems (Intuitive Surgical Inc, CA, USA) as a research platform for surgical robotics research, has been a key initiative for addressing a barrier to entry for new research groups in surgical robotics. In this paper, we present an extensive review of the publications that have been facilitated by the dVRK over the past decade. We classify research efforts into different categories and outline some of the major challenges and needs for the robotics community to maintain this initiative and build upon it.
A surgical dataset from the da Vinci Research Kit for task automation and recognition
Feb 06, 2021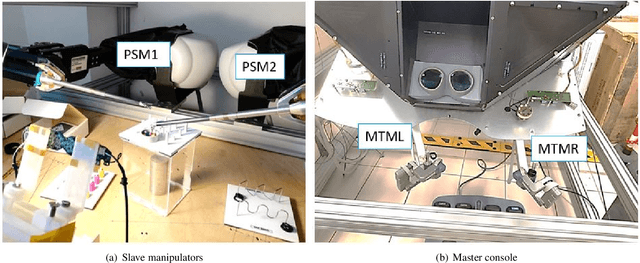
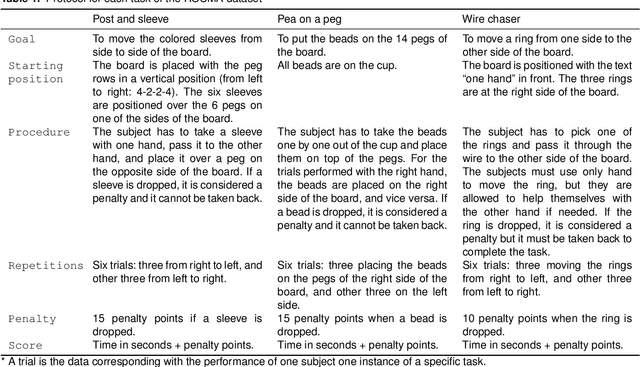
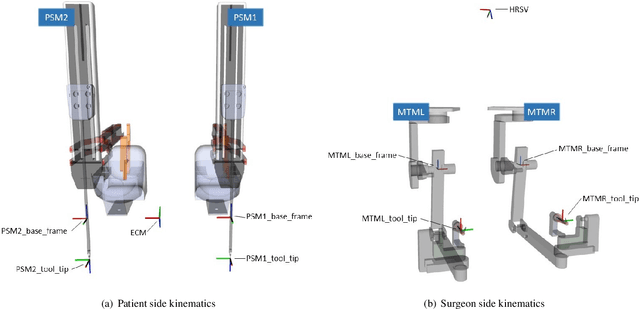

The use of datasets is getting more relevance in surgical robotics since they can be used to recognise and automate tasks. Also, this allows to use common datasets to compare different algorithms and methods. The objective of this work is to provide a complete dataset of three common training surgical tasks that surgeons perform to improve their skills. For this purpose, 12 subjects teleoperated the da Vinci Research Kit to perform these tasks. The obtained dataset includes all the kinematics and dynamics information provided by the da Vinci robot (both master and slave side) together with the associated video from the camera. All the information has been carefully timestamped and provided in a readable csv format. A MATLAB interface integrated with ROS for using and replicating the data is also provided.
Towards a Computed-Aided Diagnosis System in Colonoscopy: Automatic Polyp Segmentation Using Convolution Neural Networks
Jan 15, 2021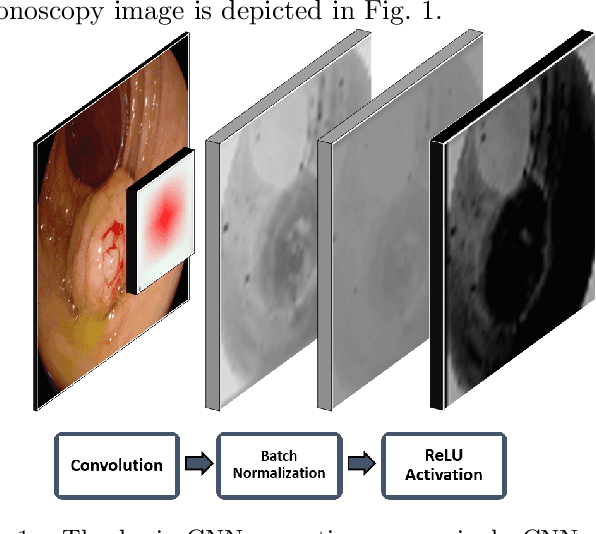
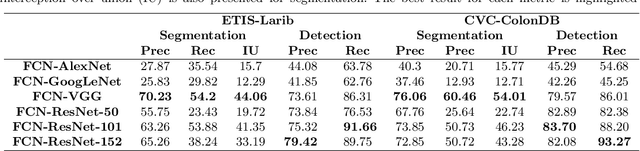
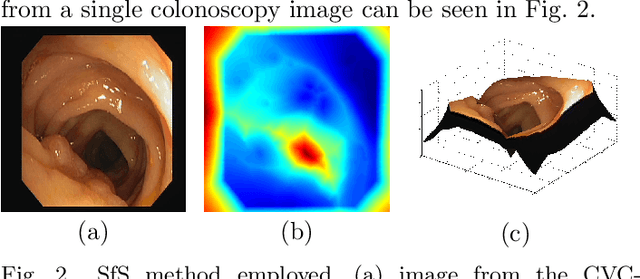

Early diagnosis is essential for the successful treatment of bowel cancers including colorectal cancer (CRC) and capsule endoscopic imaging with robotic actuation can be a valuable diagnostic tool when combined with automated image analysis. We present a deep learning rooted detection and segmentation framework for recognizing lesions in colonoscopy and capsule endoscopy images. We restructure established convolution architectures, such as VGG and ResNets, by converting them into fully-connected convolution networks (FCNs), fine-tune them and study their capabilities for polyp segmentation and detection. We additionally use Shape from-Shading (SfS) to recover depth and provide a richer representation of the tissue's structure in colonoscopy images. Depth is incorporated into our network models as an additional input channel to the RGB information and we demonstrate that the resulting network yields improved performance. Our networks are tested on publicly available datasets and the most accurate segmentation model achieved a mean segmentation IU of 47.78% and 56.95% on the ETIS-Larib and CVC-Colon datasets, respectively. For polyp detection, the top performing models we propose surpass the current state of the art with detection recalls superior to 90% for all datasets tested. To our knowledge, we present the first work to use FCNs for polyp segmentation in addition to proposing a novel combination of SfS and RGB that boosts performance
* 10 pages, 6 figures