 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeWhen CNNs Outperform Transformers and Mambas: Revisiting Deep Architectures for Dental Caries Segmentation
Nov 18, 2025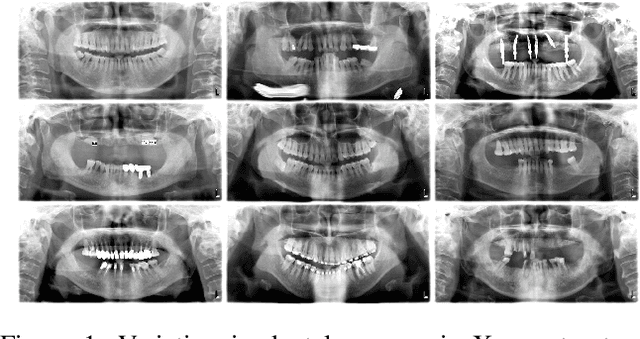
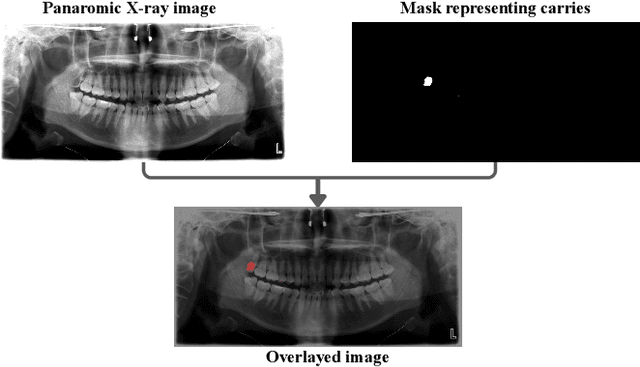
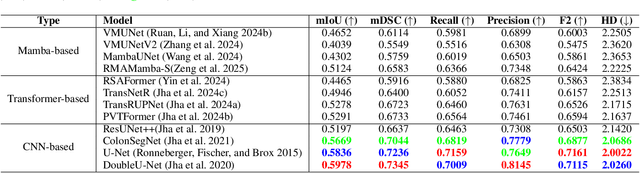
Accurate identification and segmentation of dental caries in panoramic radiographs are critical for early diagnosis and effective treatment planning. Automated segmentation remains challenging due to low lesion contrast, morphological variability, and limited annotated data. In this study, we present the first comprehensive benchmarking of convolutional neural networks, vision transformers and state-space mamba architectures for automated dental caries segmentation on panoramic radiographs through a DC1000 dataset. Twelve state-of-the-art architectures, including VMUnet, MambaUNet, VMUNetv2, RMAMamba-S, TransNetR, PVTFormer, DoubleU-Net, and ResUNet++, were trained under identical configurations. Results reveal that, contrary to the growing trend toward complex attention based architectures, the CNN-based DoubleU-Net achieved the highest dice coefficient of 0.7345, mIoU of 0.5978, and precision of 0.8145, outperforming all transformer and Mamba variants. In the study, the top 3 results across all performance metrics were achieved by CNN-based architectures. Here, Mamba and transformer-based methods, despite their theoretical advantage in global context modeling, underperformed due to limited data and weaker spatial priors. These findings underscore the importance of architecture-task alignment in domain-specific medical image segmentation more than model complexity. Our code is available at: https://github.com/JunZengz/dental-caries-segmentation.
SRMA-Mamba: Spatial Reverse Mamba Attention Network for Pathological Liver Segmentation in MRI Volumes
Aug 17, 2025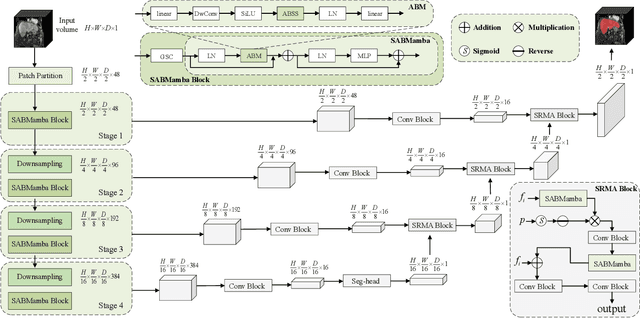

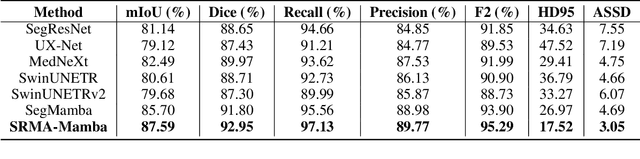
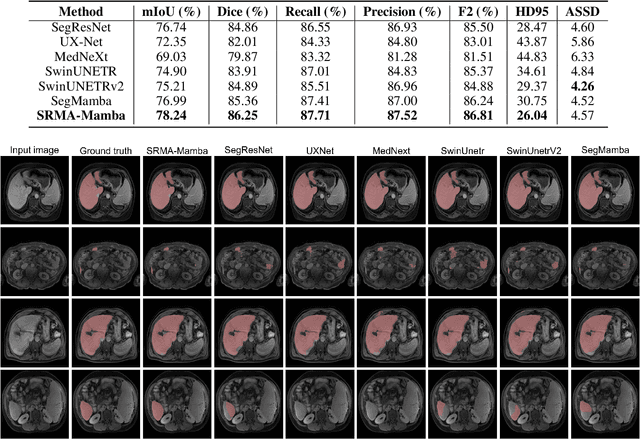
Liver Cirrhosis plays a critical role in the prognosis of chronic liver disease. Early detection and timely intervention are critical in significantly reducing mortality rates. However, the intricate anatomical architecture and diverse pathological changes of liver tissue complicate the accurate detection and characterization of lesions in clinical settings. Existing methods underutilize the spatial anatomical details in volumetric MRI data, thereby hindering their clinical effectiveness and explainability. To address this challenge, we introduce a novel Mamba-based network, SRMA-Mamba, designed to model the spatial relationships within the complex anatomical structures of MRI volumes. By integrating the Spatial Anatomy-Based Mamba module (SABMamba), SRMA-Mamba performs selective Mamba scans within liver cirrhotic tissues and combines anatomical information from the sagittal, coronal, and axial planes to construct a global spatial context representation, enabling efficient volumetric segmentation of pathological liver structures. Furthermore, we introduce the Spatial Reverse Attention module (SRMA), designed to progressively refine cirrhotic details in the segmentation map, utilizing both the coarse segmentation map and hierarchical encoding features. Extensive experiments demonstrate that SRMA-Mamba surpasses state-of-the-art methods, delivering exceptional performance in 3D pathological liver segmentation. Our code is available for public: {\color{blue}{https://github.com/JunZengz/SRMA-Mamba}}.
MDNet: Multi-Decoder Network for Abdominal CT Organs Segmentation
May 10, 2024



Accurate segmentation of organs from abdominal CT scans is essential for clinical applications such as diagnosis, treatment planning, and patient monitoring. To handle challenges of heterogeneity in organ shapes, sizes, and complex anatomical relationships, we propose a \textbf{\textit{\ac{MDNet}}}, an encoder-decoder network that uses the pre-trained \textit{MiT-B2} as the encoder and multiple different decoder networks. Each decoder network is connected to a different part of the encoder via a multi-scale feature enhancement dilated block. With each decoder, we increase the depth of the network iteratively and refine segmentation masks, enriching feature maps by integrating previous decoders' feature maps. To refine the feature map further, we also utilize the predicted masks from the previous decoder to the current decoder to provide spatial attention across foreground and background regions. MDNet effectively refines the segmentation mask with a high dice similarity coefficient (DSC) of 0.9013 and 0.9169 on the Liver Tumor segmentation (LiTS) and MSD Spleen datasets. Additionally, it reduces Hausdorff distance (HD) to 3.79 for the LiTS dataset and 2.26 for the spleen segmentation dataset, underscoring the precision of MDNet in capturing the complex contours. Moreover, \textit{\ac{MDNet}} is more interpretable and robust compared to the other baseline models.
CT Liver Segmentation via PVT-based Encoding and Refined Decoding
Jan 17, 2024


Accurate liver segmentation from CT scans is essential for computer-aided diagnosis and treatment planning. Recently, Vision Transformers achieved a competitive performance in computer vision tasks compared to convolutional neural networks due to their exceptional ability to learn global representations. However, they often struggle with scalability, memory constraints, and computational inefficiency, particularly in handling high-resolution medical images. To overcome scalability and efficiency issues, we propose a novel deep learning approach, \textit{\textbf{PVTFormer}}, that is built upon a pretrained pyramid vision transformer (PVT v2) combined with advanced residual upsampling and decoder block. By integrating a refined feature channel approach with hierarchical decoding strategy, PVTFormer generates high quality segmentation masks by enhancing semantic features. Rigorous evaluation of the proposed method on Liver Tumor Segmentation Benchmark (LiTS) 2017 demonstrates that our proposed architecture not only achieves a high dice coefficient of 86.78\%, mIoU of 78.46\%, but also obtains a low HD of 3.50. The results underscore PVTFormer's efficacy in setting a new benchmark for state-of-the-art liver segmentation methods. The source code of the proposed PVTFormer is available at \url{https://github.com/DebeshJha/PVTFormer}.
Prototype Learning for Out-of-Distribution Polyp Segmentation
Aug 07, 2023Existing polyp segmentation models from colonoscopy images often fail to provide reliable segmentation results on datasets from different centers, limiting their applicability. Our objective in this study is to create a robust and well-generalized segmentation model named PrototypeLab that can assist in polyp segmentation. To achieve this, we incorporate various lighting modes such as White light imaging (WLI), Blue light imaging (BLI), Linked color imaging (LCI), and Flexible spectral imaging color enhancement (FICE) into our new segmentation model, that learns to create prototypes for each class of object present in the images. These prototypes represent the characteristic features of the objects, such as their shape, texture, color. Our model is designed to perform effectively on out-of-distribution (OOD) datasets from multiple centers. We first generate a coarse mask that is used to learn prototypes for the main object class, which are then employed to generate the final segmentation mask. By using prototypes to represent the main class, our approach handles the variability present in the medical images and generalize well to new data since prototype capture the underlying distribution of the data. PrototypeLab offers a promising solution with a dice coefficient of $\geq$ 90\% and mIoU $\geq$ 85\% with a near real-time processing speed for polyp segmentation. It achieved superior performance on OOD datasets compared to 16 state-of-the-art image segmentation architectures, potentially improving clinical outcomes. Codes are available at https://github.com/xxxxx/PrototypeLab.
An objective validation of polyp and instrument segmentation methods in colonoscopy through Medico 2020 polyp segmentation and MedAI 2021 transparency challenges
Jul 30, 2023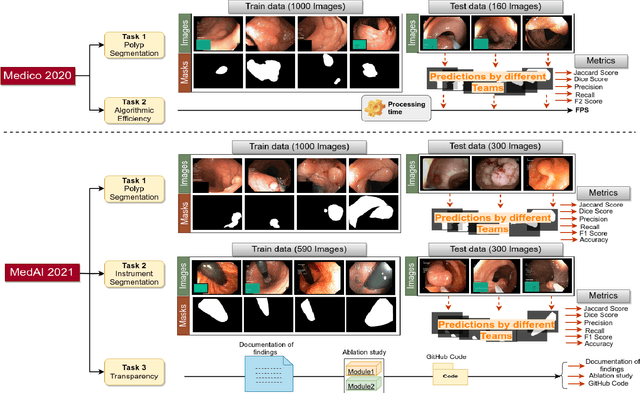
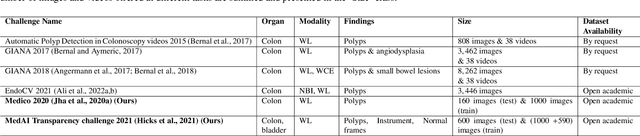
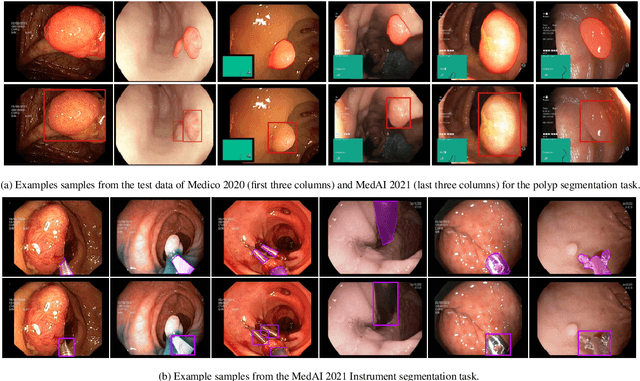
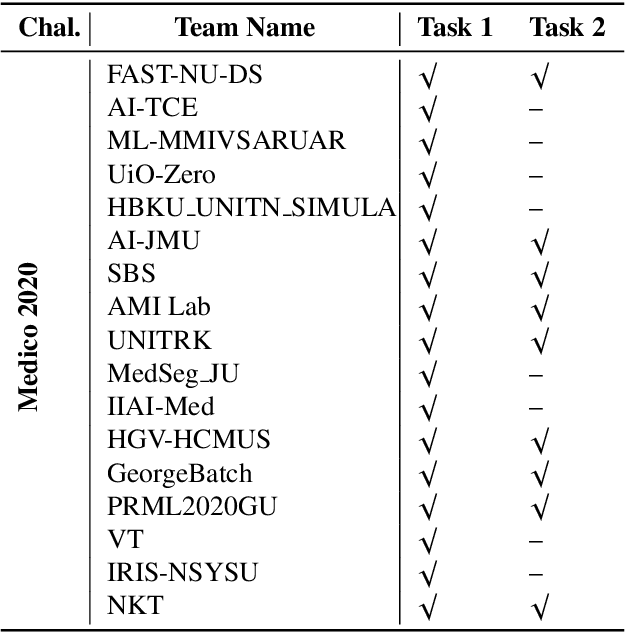
Automatic analysis of colonoscopy images has been an active field of research motivated by the importance of early detection of precancerous polyps. However, detecting polyps during the live examination can be challenging due to various factors such as variation of skills and experience among the endoscopists, lack of attentiveness, and fatigue leading to a high polyp miss-rate. Deep learning has emerged as a promising solution to this challenge as it can assist endoscopists in detecting and classifying overlooked polyps and abnormalities in real time. In addition to the algorithm's accuracy, transparency and interpretability are crucial to explaining the whys and hows of the algorithm's prediction. Further, most algorithms are developed in private data, closed source, or proprietary software, and methods lack reproducibility. Therefore, to promote the development of efficient and transparent methods, we have organized the "Medico automatic polyp segmentation (Medico 2020)" and "MedAI: Transparency in Medical Image Segmentation (MedAI 2021)" competitions. We present a comprehensive summary and analyze each contribution, highlight the strength of the best-performing methods, and discuss the possibility of clinical translations of such methods into the clinic. For the transparency task, a multi-disciplinary team, including expert gastroenterologists, accessed each submission and evaluated the team based on open-source practices, failure case analysis, ablation studies, usability and understandability of evaluations to gain a deeper understanding of the models' credibility for clinical deployment. Through the comprehensive analysis of the challenge, we not only highlight the advancements in polyp and surgical instrument segmentation but also encourage qualitative evaluation for building more transparent and understandable AI-based colonoscopy systems.
GastroVision: A Multi-class Endoscopy Image Dataset for Computer Aided Gastrointestinal Disease Detection
Jul 16, 2023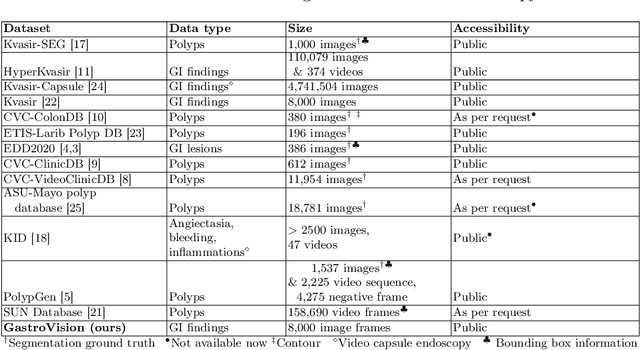
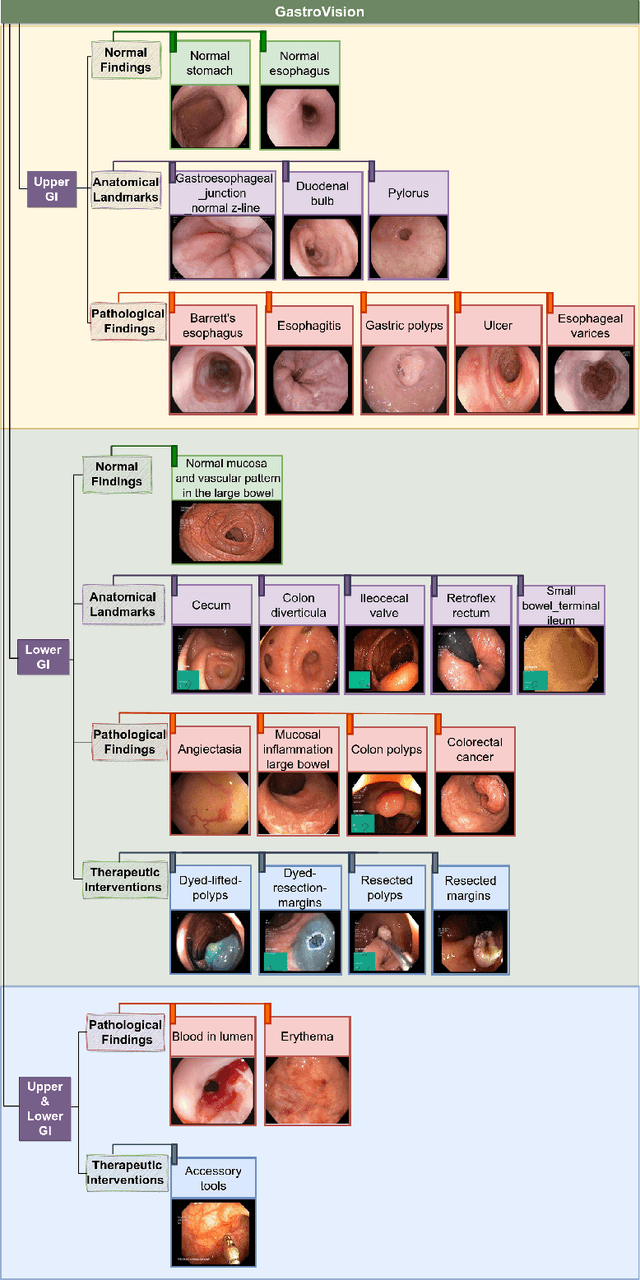
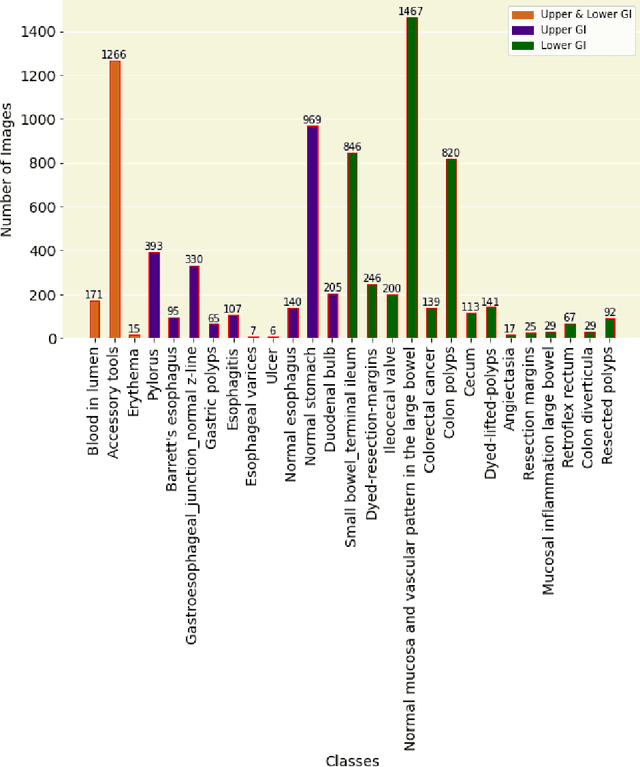
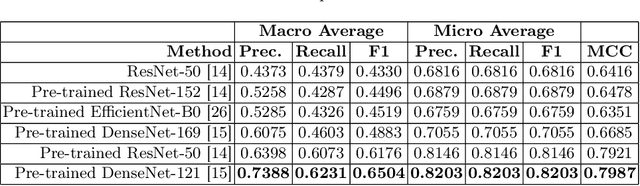
Integrating real-time artificial intelligence (AI) systems in clinical practices faces challenges such as scalability and acceptance. These challenges include data availability, biased outcomes, data quality, lack of transparency, and underperformance on unseen datasets from different distributions. The scarcity of large-scale, precisely labeled, and diverse datasets are the major challenge for clinical integration. This scarcity is also due to the legal restrictions and extensive manual efforts required for accurate annotations from clinicians. To address these challenges, we present GastroVision, a multi-center open-access gastrointestinal (GI) endoscopy dataset that includes different anatomical landmarks, pathological abnormalities, polyp removal cases and normal findings (a total of 24 classes) from the GI tract. The dataset comprises 8,000 images acquired from B{\ae}rum Hospital in Norway and Karolinska University in Sweden and was annotated and verified by experienced GI endoscopists. Furthermore, we validate the significance of our dataset with extensive benchmarking based on the popular deep learning based baseline models. We believe our dataset can facilitate the development of AI-based algorithms for GI disease detection and classification. Our dataset is available at https://osf.io/84e7f/.
TransRUPNet for Improved Out-of-Distribution Generalization in Polyp Segmentation
Jun 03, 2023Out-of-distribution (OOD) generalization is a critical challenge in deep learning. It is specifically important when the test samples are drawn from a different distribution than the training data. We develop a novel real-time deep learning based architecture, TransRUPNet that is based on a Transformer and residual upsampling network for colorectal polyp segmentation to improve OOD generalization. The proposed architecture, TransRUPNet, is an encoder-decoder network that consists of three encoder blocks, three decoder blocks, and some additional upsampling blocks at the end of the network. With the image size of $256\times256$, the proposed method achieves an excellent real-time operation speed of \textbf{47.07} frames per second with an average mean dice coefficient score of 0.7786 and mean Intersection over Union of 0.7210 on the out-of-distribution polyp datasets. The results on the publicly available PolypGen dataset (OOD dataset in our case) suggest that TransRUPNet can give real-time feedback while retaining high accuracy for in-distribution dataset. Furthermore, we demonstrate the generalizability of the proposed method by showing that it significantly improves performance on OOD datasets compared to the existing methods.
Ensuring Trustworthy Medical Artificial Intelligence through Ethical and Philosophical Principles
Apr 29, 2023Artificial intelligence (AI) methods have great potential to revolutionize numerous medical care by enhancing the experience of medical experts and patients. AI based computer-assisted diagnosis tools can have a tremendous benefit if they can outperform or perform similarly to the level of a clinical expert. As a result, advanced healthcare services can be affordable in developing nations, and the problem of a lack of expert medical practitioners can be addressed. AI based tools can save time, resources, and overall cost for patient treatment. Furthermore, in contrast to humans, AI can uncover complex relations in the data from a large set of inputs and even lead to new evidence-based knowledge in medicine. However, integrating AI in healthcare raises several ethical and philosophical concerns, such as bias, transparency, autonomy, responsibility and accountability, which must be addressed before integrating such tools into clinical settings. In this article, we emphasize recent advances in AI-assisted medical image analysis, existing standards, and the significance of comprehending ethical issues and best practices for the applications of AI in clinical settings. We cover the technical and ethical challenges of AI and the implications of deploying AI in hospitals and public organizations. We also discuss promising key measures and techniques to address the ethical challenges, data scarcity, racial bias, lack of transparency, and algorithmic bias. Finally, we provide our recommendation and future directions for addressing the ethical challenges associated with AI in healthcare applications, with the goal of deploying AI into the clinical settings to make the workflow more efficient, accurate, accessible, transparent, and reliable for the patient worldwide.
TransNetR: Transformer-based Residual Network for Polyp Segmentation with Multi-Center Out-of-Distribution Testing
Mar 13, 2023Colonoscopy is considered the most effective screening test to detect colorectal cancer (CRC) and its precursor lesions, i.e., polyps. However, the procedure experiences high miss rates due to polyp heterogeneity and inter-observer dependency. Hence, several deep learning powered systems have been proposed considering the criticality of polyp detection and segmentation in clinical practices. Despite achieving improved outcomes, the existing automated approaches are inefficient in attaining real-time processing speed. Moreover, they suffer from a significant performance drop when evaluated on inter-patient data, especially those collected from different centers. Therefore, we intend to develop a novel real-time deep learning based architecture, Transformer based Residual network (TransNetR), for colon polyp segmentation and evaluate its diagnostic performance. The proposed architecture, TransNetR, is an encoder-decoder network that consists of a pre-trained ResNet50 as the encoder, three decoder blocks, and an upsampling layer at the end of the network. TransNetR obtains a high dice coefficient of 0.8706 and a mean Intersection over union of 0.8016 and retains a real-time processing speed of 54.60 on the Kvasir-SEG dataset. Apart from this, the major contribution of the work lies in exploring the generalizability of the TransNetR by testing the proposed algorithm on the out-of-distribution (test distribution is unknown and different from training distribution) dataset. As a use case, we tested our proposed algorithm on the PolypGen (6 unique centers) dataset and two other popular polyp segmentation benchmarking datasets. We obtained state-of-the-art performance on all three datasets during out-of-distribution testing. The source code of TransNetR will be made publicly available at https://github.com/DebeshJha.