 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeMaximizing T2-Only Prostate Cancer Localization from Expected Diffusion Weighted Imaging
Apr 01, 2026Multiparametric MRI is increasingly recommended as a first-line noninvasive approach to detect and localize prostate cancer, requiring at minimum diffusion-weighted (DWI) and T2-weighted (T2w) MR sequences. Early machine learning attempts using only T2w images have shown promising diagnostic performance in segmenting radiologist-annotated lesions. Such uni-modal T2-only approaches deliver substantial clinical benefits by reducing costs and expertise required to acquire other sequences. This work investigates an arguably more challenging application using only T2w at inference, but to localize individual cancers based on independent histopathology labels. We formulate DWI images as a latent modality (readily available during training) to classify cancer presence at local Barzell zones, given only T2w images as input. In the resulting expectation-maximization algorithm, a latent modality generator (implemented using a flow matching-based generative model) approximates the latent DWI image posterior distribution in the E-steps, while in M-steps a cancer localizer is simultaneously optimized with the generative model to maximize the expected likelihood of cancer presence. The proposed approach provides a novel theoretical framework for learning from a privileged DWI modality, yielding superior cancer localization performance compared to approaches that lack training DWI images or existing frameworks for privileged learning and incomplete modalities. The proposed T2-only methods perform competitively or better than baseline methods using multiple input sequences (e.g., improving the patient-level F1 score by 14.4\% and zone-level QWK by 5.3\% over the T2w+DWI baseline). We present quantitative evaluations using internal and external datasets from 4,133 prostate cancer patients with histopathology-verified labels.
On the Degrees of Freedom of Gridded Control Points in Learning-Based Medical Image Registration
Mar 15, 2026Many registration problems are ill-posed in homogeneous or noisy regions, and dense voxel-wise decoders can be unnecessarily high-dimensional. A sparse control-point parameterisation provides a compact, smooth deformation representation while reducing memory and improving stability. This work investigates the required control points for learning-based registration network development. We present GridReg, a learning-based registration framework that replaces dense voxel-wise decoding with displacement predictions at a sparse grid of control points. This design substantially cuts the parameter count and memory while retaining registration accuracy. Multiscale 3D encoder feature maps are flattened into a 1D token sequence with positional encoding to retain spatial context. The model then predicts a sparse gridded deformation field using a cross-attention module. We further introduce grid-adaptive training, enabling an adaptive model to operate at multiple grid sizes at inference without retraining. This work quantitatively demonstrates the benefits of using sparse grids. Using three data sets for registering prostate gland, pelvic organs and neurological structures, the results suggested a significant improvement with the usage of grid-controled displacement field. Alternatively, the superior registration performance was obtained using the proposed approach, with a similar or less computational cost, compared with existing algorithms that predict DDFs or displacements sampled on scattered key points.
ProFound: A moderate-sized vision foundation model for multi-task prostate imaging
Mar 04, 2026Many diagnostic and therapeutic clinical tasks for prostate cancer increasingly rely on multi-parametric MRI. Automating these tasks is challenging because they necessitate expert interpretations, which are difficult to scale to capitalise on modern deep learning. Although modern automated systems achieve expert-level performance in isolated tasks, their general clinical utility remains limited by the requirement of large task-specific labelled datasets. In this paper, we present ProFound, a domain-specialised vision foundation model for volumetric prostate mpMRI. ProFound is pre-trained using several variants of self-supervised approaches on a diverse, multi-institutional collection of 5,000 patients, with a total of over 22,000 unique 3D MRI volumes (over 1,800,000 2D image slices). We conducted a systematic evaluation of ProFound across a broad spectrum of $11$ downstream clinical tasks on over 3,000 independent patients, including prostate cancer detection, Gleason grading, lesion localisation, gland volume estimation, zonal and surrounding structure segmentation. Experimental results demonstrate that finetuned ProFound consistently outperforms or remains competitive with state-of-the-art specialised models and existing medical vision foundation models trained/finetuned on the same data.
Understanding the Transfer Limits of Vision Foundation Models
Jan 22, 2026Foundation models leverage large-scale pretraining to capture extensive knowledge, demonstrating generalization in a wide range of language tasks. By comparison, vision foundation models (VFMs) often exhibit uneven improvements across downstream tasks, despite substantial computational investment. We postulate that this limitation arises from a mismatch between pretraining objectives and the demands of downstream vision-and-imaging tasks. Pretraining strategies like masked image reconstruction or contrastive learning shape representations for tasks such as recovery of generic visual patterns or global semantic structures, which may not align with the task-specific requirements of downstream applications including segmentation, classification, or image synthesis. To investigate this in a concrete real-world clinical area, we assess two VFMs, a reconstruction-focused MAE-based model (ProFound) and a contrastive-learning-based model (ProViCNet), on five prostate multiparametric MR imaging tasks, examining how such task alignment influences transfer performance, i.e., from pretraining to fine-tuning. Our findings indicate that better alignment between pretraining and downstream tasks, measured by simple divergence metrics such as maximum-mean-discrepancy (MMD) between the same features before and after fine-tuning, correlates with greater performance improvements and faster convergence, emphasizing the importance of designing and analyzing pretraining objectives with downstream applicability in mind.
Dual Deep Learning Approach for Non-invasive Renal Tumour Subtyping with VERDICT-MRI
Apr 09, 2025This work aims to characterise renal tumour microstructure using diffusion MRI (dMRI); via the Vascular, Extracellular and Restricted Diffusion for Cytometry in Tumours (VERDICT)-MRI framework with self-supervised learning. Comprehensive datasets were acquired from 14 patients with 15 biopsy-confirmed renal tumours, with nine b-values in the range b=[0,2500]s/mm2. A three-compartment VERDICT model for renal tumours was fitted to the dMRI data using a self-supervised deep neural network, and ROIs were drawn by an experienced uroradiologist. An economical acquisition protocol for future studies with larger patient cohorts was optimised using a recursive feature selection approach. The VERDICT model described the diffusion data in renal tumours more accurately than IVIM or ADC. Combined with self-supervised deep learning, VERDICT identified significant differences in the intracellular volume fraction between cancerous and normal tissue, and in the vascular volume fraction between vascular and non-vascular. The feature selector yields a 4 b-value acquisition of b = [70,150,1000,2000], with a duration of 14 minutes.
Tell2Reg: Establishing spatial correspondence between images by the same language prompts
Feb 05, 2025Spatial correspondence can be represented by pairs of segmented regions, such that the image registration networks aim to segment corresponding regions rather than predicting displacement fields or transformation parameters. In this work, we show that such a corresponding region pair can be predicted by the same language prompt on two different images using the pre-trained large multimodal models based on GroundingDINO and SAM. This enables a fully automated and training-free registration algorithm, potentially generalisable to a wide range of image registration tasks. In this paper, we present experimental results using one of the challenging tasks, registering inter-subject prostate MR images, which involves both highly variable intensity and morphology between patients. Tell2Reg is training-free, eliminating the need for costly and time-consuming data curation and labelling that was previously required for this registration task. This approach outperforms unsupervised learning-based registration methods tested, and has a performance comparable to weakly-supervised methods. Additional qualitative results are also presented to suggest that, for the first time, there is a potential correlation between language semantics and spatial correspondence, including the spatial invariance in language-prompted regions and the difference in language prompts between the obtained local and global correspondences. Code is available at https://github.com/yanwenCi/Tell2Reg.git.
T2-Only Prostate Cancer Prediction by Meta-Learning from Bi-Parametric MR Imaging
Nov 11, 2024


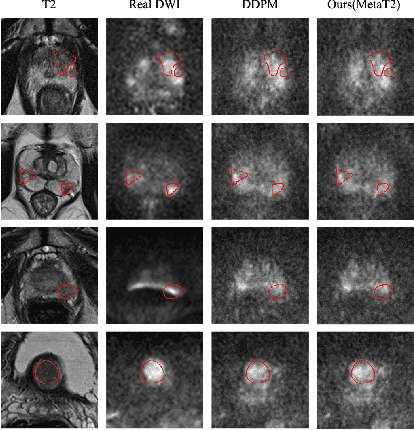
Current imaging-based prostate cancer diagnosis requires both MR T2-weighted (T2w) and diffusion-weighted imaging (DWI) sequences, with additional sequences for potentially greater accuracy improvement. However, measuring diffusion patterns in DWI sequences can be time-consuming, prone to artifacts and sensitive to imaging parameters. While machine learning (ML) models have demonstrated radiologist-level accuracy in detecting prostate cancer from these two sequences, this study investigates the potential of ML-enabled methods using only the T2w sequence as input during inference time. We first discuss the technical feasibility of such a T2-only approach, and then propose a novel ML formulation, where DWI sequences - readily available for training purposes - are only used to train a meta-learning model, which subsequently only uses T2w sequences at inference. Using multiple datasets from more than 3,000 prostate cancer patients, we report superior or comparable performance in localising radiologist-identified prostate cancer using our proposed T2-only models, compared with alternative models using T2-only or both sequences as input. Real patient cases are presented and discussed to demonstrate, for the first time, the exclusively true-positive cases from models with different input sequences.
AI-assisted prostate cancer detection and localisation on biparametric MR by classifying radiologist-positives
Oct 30, 2024



Prostate cancer diagnosis through MR imaging have currently relied on radiologists' interpretation, whilst modern AI-based methods have been developed to detect clinically significant cancers independent of radiologists. In this study, we propose to develop deep learning models that improve the overall cancer diagnostic accuracy, by classifying radiologist-identified patients or lesions (i.e. radiologist-positives), as opposed to the existing models that are trained to discriminate over all patients. We develop a single voxel-level classification model, with a simple percentage threshold to determine positive cases, at levels of lesions, Barzell-zones and patients. Based on the presented experiments from two clinical data sets, consisting of histopathology-labelled MR images from more than 800 and 500 patients in the respective UCLA and UCL PROMIS studies, we show that the proposed strategy can improve the diagnostic accuracy, by augmenting the radiologist reading of the MR imaging. Among varying definition of clinical significance, the proposed strategy, for example, achieved a specificity of 44.1% (with AI assistance) from 36.3% (by radiologists alone), at a controlled sensitivity of 80.0% on the publicly available UCLA data set. This provides measurable clinical values in a range of applications such as reducing unnecessary biopsies, lowering cost in cancer screening and quantifying risk in therapies.
Poisson Ordinal Network for Gleason Group Estimation Using Bi-Parametric MRI
Jul 08, 2024



The Gleason groups serve as the primary histological grading system for prostate cancer, providing crucial insights into the cancer's potential for growth and metastasis. In clinical practice, pathologists determine the Gleason groups based on specimens obtained from ultrasound-guided biopsies. In this study, we investigate the feasibility of directly estimating the Gleason groups from MRI scans to reduce otherwise required biopsies. We identify two characteristics of this task, ordinality and the resulting dependent yet unknown variances between Gleason groups. In addition to the inter- / intra- observer variability in a multi-step Gleason scoring process based on the interpretation of Gleason patterns, our MR-based prediction is also subject to specimen sampling variance and, to a lesser degree, varying MR imaging protocols. To address this challenge, we propose a novel Poisson ordinal network (PON). PONs model the prediction using a Poisson distribution and leverages Poisson encoding and Poisson focal loss to capture a learnable dependency between ordinal classes (here, Gleason groups), rather than relying solely on the numerical ground-truth (e.g. Gleason Groups 1-5 or Gleason Scores 6-10). To improve this modelling efficacy, PONs also employ contrastive learning with a memory bank to regularise intra-class variance, decoupling the memory requirement of contrast learning from the batch size. Experimental results based on the images labelled by saturation biopsies from 265 prior-biopsy-blind patients, across two tasks demonstrate the superiority and effectiveness of our proposed method.
ssVERDICT: Self-Supervised VERDICT-MRI for Enhanced Prostate Tumour Characterisation
Sep 27, 2023
Purpose: Demonstrating and assessing self-supervised machine learning fitting of the VERDICT (Vascular, Extracellular and Restricted DIffusion for Cytometry in Tumours) model for prostate. Methods: We derive a self-supervised neural network for fitting VERDICT (ssVERDICT) that estimates parameter maps without training data. We compare the performance of ssVERDICT to two established baseline methods for fitting diffusion MRI models: conventional nonlinear least squares (NLLS) and supervised deep learning. We do this quantitatively on simulated data, by comparing the Pearson's correlation coefficient, mean-squared error (MSE), bias, and variance with respect to the simulated ground truth. We also calculate in vivo parameter maps on a cohort of 20 prostate cancer patients and compare the methods' performance in discriminating benign from cancerous tissue via Wilcoxon's signed-rank test. Results: In simulations, ssVERDICT outperforms the baseline methods (NLLS and supervised DL) in estimating all the parameters from the VERDICT prostate model in terms of Pearson's correlation coefficient, bias, and MSE. In vivo, ssVERDICT shows stronger lesion conspicuity across all parameter maps, and improves discrimination between benign and cancerous tissue over the baseline methods. Conclusion: ssVERDICT significantly outperforms state-of-the-art methods for VERDICT model fitting, and shows for the first time, fitting of a complex three-compartment biophysical model with machine learning without the requirement of explicit training labels.