 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeUnderstanding the Transfer Limits of Vision Foundation Models
Jan 22, 2026Foundation models leverage large-scale pretraining to capture extensive knowledge, demonstrating generalization in a wide range of language tasks. By comparison, vision foundation models (VFMs) often exhibit uneven improvements across downstream tasks, despite substantial computational investment. We postulate that this limitation arises from a mismatch between pretraining objectives and the demands of downstream vision-and-imaging tasks. Pretraining strategies like masked image reconstruction or contrastive learning shape representations for tasks such as recovery of generic visual patterns or global semantic structures, which may not align with the task-specific requirements of downstream applications including segmentation, classification, or image synthesis. To investigate this in a concrete real-world clinical area, we assess two VFMs, a reconstruction-focused MAE-based model (ProFound) and a contrastive-learning-based model (ProViCNet), on five prostate multiparametric MR imaging tasks, examining how such task alignment influences transfer performance, i.e., from pretraining to fine-tuning. Our findings indicate that better alignment between pretraining and downstream tasks, measured by simple divergence metrics such as maximum-mean-discrepancy (MMD) between the same features before and after fine-tuning, correlates with greater performance improvements and faster convergence, emphasizing the importance of designing and analyzing pretraining objectives with downstream applicability in mind.
Tell2Reg: Establishing spatial correspondence between images by the same language prompts
Feb 05, 2025Spatial correspondence can be represented by pairs of segmented regions, such that the image registration networks aim to segment corresponding regions rather than predicting displacement fields or transformation parameters. In this work, we show that such a corresponding region pair can be predicted by the same language prompt on two different images using the pre-trained large multimodal models based on GroundingDINO and SAM. This enables a fully automated and training-free registration algorithm, potentially generalisable to a wide range of image registration tasks. In this paper, we present experimental results using one of the challenging tasks, registering inter-subject prostate MR images, which involves both highly variable intensity and morphology between patients. Tell2Reg is training-free, eliminating the need for costly and time-consuming data curation and labelling that was previously required for this registration task. This approach outperforms unsupervised learning-based registration methods tested, and has a performance comparable to weakly-supervised methods. Additional qualitative results are also presented to suggest that, for the first time, there is a potential correlation between language semantics and spatial correspondence, including the spatial invariance in language-prompted regions and the difference in language prompts between the obtained local and global correspondences. Code is available at https://github.com/yanwenCi/Tell2Reg.git.
Biomechanics-informed Non-rigid Medical Image Registration and its Inverse Material Property Estimation with Linear and Nonlinear Elasticity
Jul 03, 2024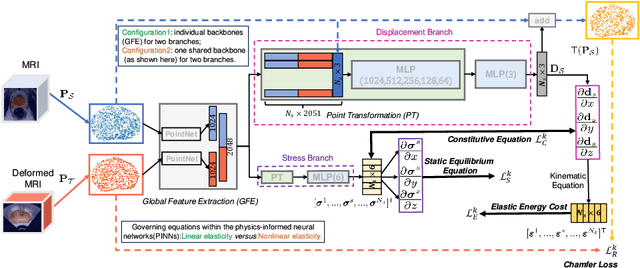
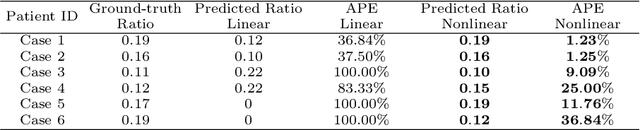
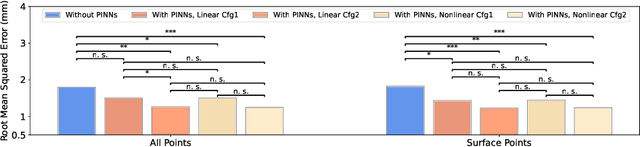
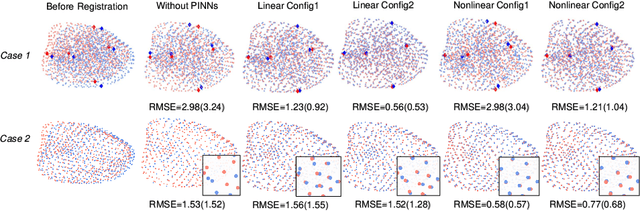
This paper investigates both biomechanical-constrained non-rigid medical image registrations and accurate identifications of material properties for soft tissues, using physics-informed neural networks (PINNs). The complex nonlinear elasticity theory is leveraged to formally establish the partial differential equations (PDEs) representing physics laws of biomechanical constraints that need to be satisfied, with which registration and identification tasks are treated as forward (i.e., data-driven solutions of PDEs) and inverse (i.e., parameter estimation) problems under PINNs respectively. Two net configurations (i.e., Cfg1 and Cfg2) have also been compared for both linear and nonlinear physics model. Two sets of experiments have been conducted, using pairs of undeformed and deformed MR images from clinical cases of prostate cancer biopsy. Our contributions are summarised as follows. 1) We developed a learning-based biomechanical-constrained non-rigid registration algorithm using PINNs, where linear elasticity is generalised to the nonlinear version. 2) We demonstrated extensively that nonlinear elasticity shows no statistical significance against linear models in computing point-wise displacement vectors but their respective benefits may depend on specific patients, with finite-element (FE) computed ground-truth. 3) We formulated and solved the inverse parameter estimation problem, under the joint optimisation scheme of registration and parameter identification using PINNs, whose solutions can be accurately found by locating saddle points.
Weakly supervised localisation of prostate cancer using reinforcement learning for bi-parametric MR images
Feb 21, 2024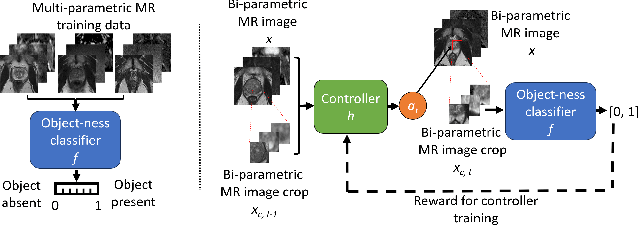
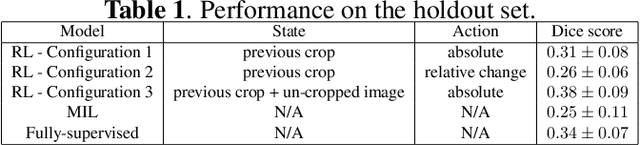
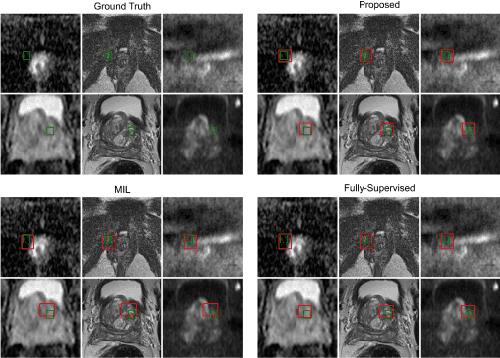
In this paper we propose a reinforcement learning based weakly supervised system for localisation. We train a controller function to localise regions of interest within an image by introducing a novel reward definition that utilises non-binarised classification probability, generated by a pre-trained binary classifier which classifies object presence in images or image crops. The object-presence classifier may then inform the controller of its localisation quality by quantifying the likelihood of the image containing an object. Such an approach allows us to minimize any potential labelling or human bias propagated via human labelling for fully supervised localisation. We evaluate our proposed approach for a task of cancerous lesion localisation on a large dataset of real clinical bi-parametric MR images of the prostate. Comparisons to the commonly used multiple-instance learning weakly supervised localisation and to a fully supervised baseline show that our proposed method outperforms the multi-instance learning and performs comparably to fully-supervised learning, using only image-level classification labels for training.
Semi-weakly-supervised neural network training for medical image registration
Feb 16, 2024



For training registration networks, weak supervision from segmented corresponding regions-of-interest (ROIs) have been proven effective for (a) supplementing unsupervised methods, and (b) being used independently in registration tasks in which unsupervised losses are unavailable or ineffective. This correspondence-informing supervision entails cost in annotation that requires significant specialised effort. This paper describes a semi-weakly-supervised registration pipeline that improves the model performance, when only a small corresponding-ROI-labelled dataset is available, by exploiting unlabelled image pairs. We examine two types of augmentation methods by perturbation on network weights and image resampling, such that consistency-based unsupervised losses can be applied on unlabelled data. The novel WarpDDF and RegCut approaches are proposed to allow commutative perturbation between an image pair and the predicted spatial transformation (i.e. respective input and output of registration networks), distinct from existing perturbation methods for classification or segmentation. Experiments using 589 male pelvic MR images, labelled with eight anatomical ROIs, show the improvement in registration performance and the ablated contributions from the individual strategies. Furthermore, this study attempts to construct one of the first computational atlases for pelvic structures, enabled by registering inter-subject MRs, and quantifies the significant differences due to the proposed semi-weak supervision with a discussion on the potential clinical use of example atlas-derived statistics.
Combiner and HyperCombiner Networks: Rules to Combine Multimodality MR Images for Prostate Cancer Localisation
Jul 17, 2023



One of the distinct characteristics in radiologists' reading of multiparametric prostate MR scans, using reporting systems such as PI-RADS v2.1, is to score individual types of MR modalities, T2-weighted, diffusion-weighted, and dynamic contrast-enhanced, and then combine these image-modality-specific scores using standardised decision rules to predict the likelihood of clinically significant cancer. This work aims to demonstrate that it is feasible for low-dimensional parametric models to model such decision rules in the proposed Combiner networks, without compromising the accuracy of predicting radiologic labels: First, it is shown that either a linear mixture model or a nonlinear stacking model is sufficient to model PI-RADS decision rules for localising prostate cancer. Second, parameters of these (generalised) linear models are proposed as hyperparameters, to weigh multiple networks that independently represent individual image modalities in the Combiner network training, as opposed to end-to-end modality ensemble. A HyperCombiner network is developed to train a single image segmentation network that can be conditioned on these hyperparameters during inference, for much improved efficiency. Experimental results based on data from 850 patients, for the application of automating radiologist labelling multi-parametric MR, compare the proposed combiner networks with other commonly-adopted end-to-end networks. Using the added advantages of obtaining and interpreting the modality combining rules, in terms of the linear weights or odds-ratios on individual image modalities, three clinical applications are presented for prostate cancer segmentation, including modality availability assessment, importance quantification and rule discovery.
A hybrid CNN-RNN approach for survival analysis in a Lung Cancer Screening study
Mar 19, 2023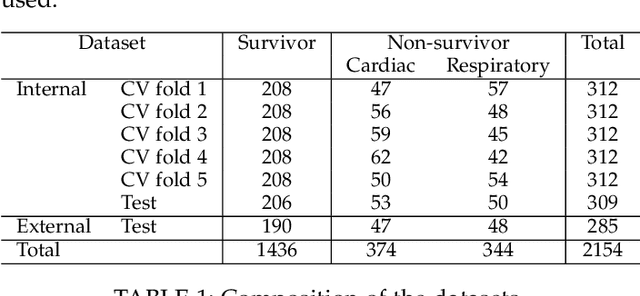


In this study, we present a hybrid CNN-RNN approach to investigate long-term survival of subjects in a lung cancer screening study. Subjects who died of cardiovascular and respiratory causes were identified whereby the CNN model was used to capture imaging features in the CT scans and the RNN model was used to investigate time series and thus global information. The models were trained on subjects who underwent cardiovascular and respiratory deaths and a control cohort matched to participant age, gender, and smoking history. The combined model can achieve an AUC of 0.76 which outperforms humans at cardiovascular mortality prediction. The corresponding F1 and Matthews Correlation Coefficient are 0.63 and 0.42 respectively. The generalisability of the model is further validated on an 'external' cohort. The same models were applied to survival analysis with the Cox Proportional Hazard model. It was demonstrated that incorporating the follow-up history can lead to improvement in survival prediction. The Cox neural network can achieve an IPCW C-index of 0.75 on the internal dataset and 0.69 on an external dataset. Delineating imaging features associated with long-term survival can help focus preventative interventions appropriately, particularly for under-recognised pathologies thereby potentially reducing patient morbidity.
Bi-parametric prostate MR image synthesis using pathology and sequence-conditioned stable diffusion
Mar 03, 2023We propose an image synthesis mechanism for multi-sequence prostate MR images conditioned on text, to control lesion presence and sequence, as well as to generate paired bi-parametric images conditioned on images e.g. for generating diffusion-weighted MR from T2-weighted MR for paired data, which are two challenging tasks in pathological image synthesis. Our proposed mechanism utilises and builds upon the recent stable diffusion model by proposing image-based conditioning for paired data generation. We validate our method using 2D image slices from real suspected prostate cancer patients. The realism of the synthesised images is validated by means of a blind expert evaluation for identifying real versus fake images, where a radiologist with 4 years experience reading urological MR only achieves 59.4% accuracy across all tested sequences (where chance is 50%). For the first time, we evaluate the realism of the generated pathology by blind expert identification of the presence of suspected lesions, where we find that the clinician performs similarly for both real and synthesised images, with a 2.9 percentage point difference in lesion identification accuracy between real and synthesised images, demonstrating the potentials in radiological training purposes. Furthermore, we also show that a machine learning model, trained for lesion identification, shows better performance (76.2% vs 70.4%, statistically significant improvement) when trained with real data augmented by synthesised data as opposed to training with only real images, demonstrating usefulness for model training.
Non-rigid Medical Image Registration using Physics-informed Neural Networks
Feb 20, 2023



Biomechanical modelling of soft tissue provides a non-data-driven method for constraining medical image registration, such that the estimated spatial transformation is considered biophysically plausible. This has not only been adopted in real-world clinical applications, such as the MR-to-ultrasound registration for prostate intervention of interest in this work, but also provides an explainable means of understanding the organ motion and spatial correspondence establishment. This work instantiates the recently-proposed physics-informed neural networks (PINNs) to a 3D linear elastic model for modelling prostate motion commonly encountered during transrectal ultrasound guided procedures. To overcome a widely-recognised challenge in generalising PINNs to different subjects, we propose to use PointNet as the nodal-permutation-invariant feature extractor, together with a registration algorithm that aligns point sets and simultaneously takes into account the PINN-imposed biomechanics. The proposed method has been both developed and validated in both patient-specific and multi-patient manner.
Prototypical few-shot segmentation for cross-institution male pelvic structures with spatial registration
Sep 13, 2022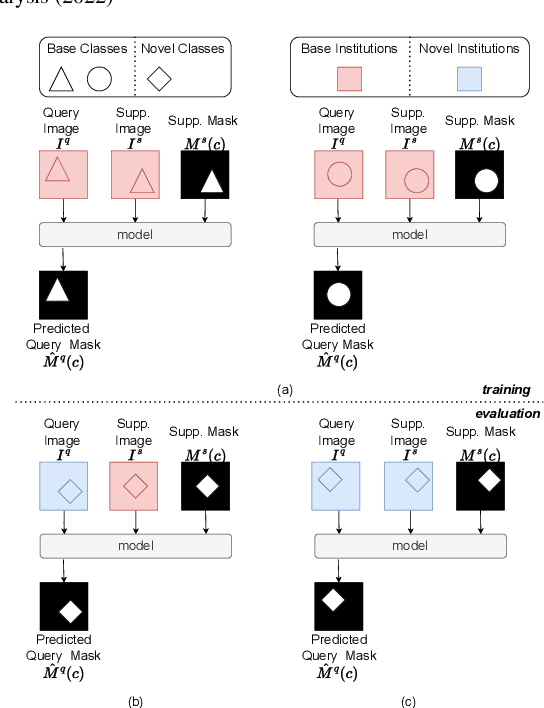
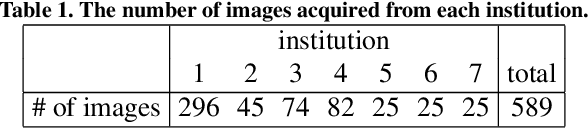
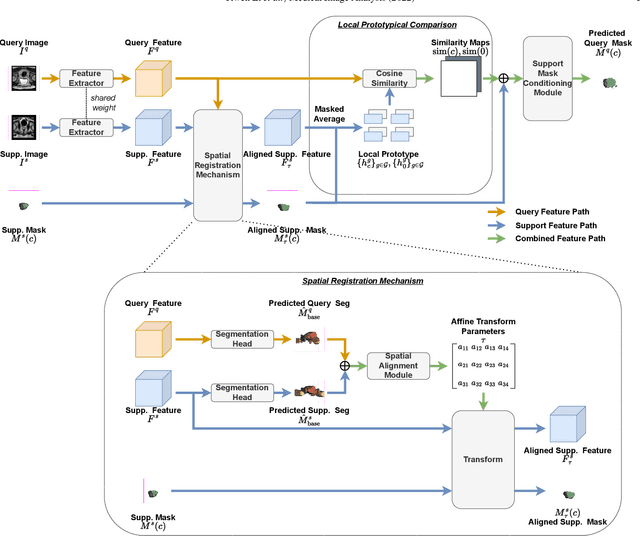
The prowess that makes few-shot learning desirable in medical image analysis is the efficient use of the support image data, which are labelled to classify or segment new classes, a task that otherwise requires substantially more training images and expert annotations. This work describes a fully 3D prototypical few-shot segmentation algorithm, such that the trained networks can be effectively adapted to clinically interesting structures that are absent in training, using only a few labelled images from a different institute. First, to compensate for the widely recognised spatial variability between institutions in episodic adaptation of novel classes, a novel spatial registration mechanism is integrated into prototypical learning, consisting of a segmentation head and an spatial alignment module. Second, to assist the training with observed imperfect alignment, support mask conditioning module is proposed to further utilise the annotation available from the support images. Extensive experiments are presented in an application of segmenting eight anatomical structures important for interventional planning, using a data set of 589 pelvic T2-weighted MR images, acquired at seven institutes. The results demonstrate the efficacy in each of the 3D formulation, the spatial registration, and the support mask conditioning, all of which made positive contributions independently or collectively. Compared with the previously proposed 2D alternatives, the few-shot segmentation performance was improved with statistical significance, regardless whether the support data come from the same or different institutes.