 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeSingle-Rollout Hidden-State Dynamics for Training-Free RLVR Data Selection
May 27, 2026Reinforcement learning with verifiable rewards (RLVR) can yield large reasoning gains from very few training instances, yet its strong sensitivity to which instances are used makes data selection a central bottleneck. Most existing selection pipelines rely on training-time optimization signals and/or require access to verifiable rewards or ground-truth answers over large candidate pools, which is costly and often infeasible in specialized domains. We study RLVR data selection in a setting where selection must be performed before any RL training and without labels or reward evaluation on the full pool. We propose SHIFT, a one-shot, training-free selector based solely on inference-time hidden-state dynamics. For each candidate instance, SHIFT runs a single deterministic reasoning rollout and computes a reasoning-induced representation shift (RIRS) as the start-to-end hidden-state delta. SHIFT uses the RIRS magnitude as a lightweight proxy for instance utility and enforces coverage via a quality-weighted farthest-first CoreSet procedure in an RIRS-augmented feature space, producing compact subsets that scale to large unlabeled pools. Across mathematical reasoning and medical QA benchmarks under ultra-low budgets, SHIFT consistently outperforms training-free diversity and difficulty/uncertainty baselines, improving both in-domain accuracy and transfer to harder evaluation settings. Ablations show that RIRS-based coverage and quality-weighting contribute complementary gains, and analyses indicate that RIRS is not explained by simple input/output length statistics. Code is available at github.com/JianghaoWu/SHIFT.
RAFM: Retrieval-Augmented Flow Matching for Unpaired CBCT-to-CT Translation
Feb 28, 2026Cone-beam CT (CBCT) is routinely acquired in radiotherapy but suffers from severe artifacts and unreliable Hounsfield Unit (HU) values, limiting its direct use for dose calculation. Synthetic CT (sCT) generation from CBCT is therefore an important task, yet paired CBCT--CT data are often unavailable or unreliable due to temporal gaps, anatomical variation, and registration errors. In this work, we introduce rectified flow (RF) into unpaired CBCT-to-CT translation in medical imaging. Although RF is theoretically compatible with unpaired learning through distribution-level coupling and deterministic transport, its practical effectiveness under small medical datasets and limited batch sizes remains underexplored. Direct application with random or batch-local pseudo pairing can produce unstable supervision due to semantically mismatched endpoint samples. To address this challenge, we propose Retrieval-Augmented Flow Matching (RAFM), which adapts RF to the medical setting by constructing retrieval-guided pseudo pairs using a frozen DINOv3 encoder and a global CT memory bank. This strategy improves empirical coupling quality and stabilizes unpaired flow-based training. Experiments on SynthRAD2023 under a strict subject-level true-unpaired protocol show that RAFM outperforms existing methods across FID, MAE, SSIM, PSNR, and SegScore. The code is available at https://github.com/HiLab-git/RAFM.git.
A3-TTA: Adaptive Anchor Alignment Test-Time Adaptation for Image Segmentation
Feb 03, 2026Test-Time Adaptation (TTA) offers a practical solution for deploying image segmentation models under domain shift without accessing source data or retraining. Among existing TTA strategies, pseudo-label-based methods have shown promising performance. However, they often rely on perturbation-ensemble heuristics (e.g., dropout sampling, test-time augmentation, Gaussian noise), which lack distributional grounding and yield unstable training signals. This can trigger error accumulation and catastrophic forgetting during adaptation. To address this, we propose \textbf{A3-TTA}, a TTA framework that constructs reliable pseudo-labels through anchor-guided supervision. Specifically, we identify well-predicted target domain images using a class compact density metric, under the assumption that confident predictions imply distributional proximity to the source domain. These anchors serve as stable references to guide pseudo-label generation, which is further regularized via semantic consistency and boundary-aware entropy minimization. Additionally, we introduce a self-adaptive exponential moving average strategy to mitigate label noise and stabilize model update during adaptation. Evaluated on both multi-domain medical images (heart structure and prostate segmentation) and natural images, A3-TTA significantly improves average Dice scores by 10.40 to 17.68 percentage points compared to the source model, outperforming several state-of-the-art TTA methods under different segmentation model architectures. A3-TTA also excels in continual TTA, maintaining high performance across sequential target domains with strong anti-forgetting ability. The code will be made publicly available at https://github.com/HiLab-git/A3-TTA.
SegRap2025: A Benchmark of Gross Tumor Volume and Lymph Node Clinical Target Volume Segmentation for Radiotherapy Planning of Nasopharyngeal Carcinoma
Jan 28, 2026Accurate delineation of Gross Tumor Volume (GTV), Lymph Node Clinical Target Volume (LN CTV), and Organ-at-Risk (OAR) from Computed Tomography (CT) scans is essential for precise radiotherapy planning in Nasopharyngeal Carcinoma (NPC). Building upon SegRap2023, which focused on OAR and GTV segmentation using single-center paired non-contrast CT (ncCT) and contrast-enhanced CT (ceCT) scans, the SegRap2025 challenge aims to enhance the generalizability and robustness of segmentation models across imaging centers and modalities. SegRap2025 comprises two tasks: Task01 addresses GTV segmentation using paired CT from the SegRap2023 dataset, with an additional external testing set to evaluate cross-center generalization, and Task02 focuses on LN CTV segmentation using multi-center training data and an unseen external testing set, where each case contains paired CT scans or a single modality, emphasizing both cross-center and cross-modality robustness. This paper presents the challenge setup and provides a comprehensive analysis of the solutions submitted by ten participating teams. For GTV segmentation task, the top-performing models achieved average Dice Similarity Coefficient (DSC) of 74.61% and 56.79% on the internal and external testing cohorts, respectively. For LN CTV segmentation task, the highest average DSC values reached 60.24%, 60.50%, and 57.23% on paired CT, ceCT-only, and ncCT-only subsets, respectively. SegRap2025 establishes a large-scale multi-center, multi-modality benchmark for evaluating the generalization and robustness in radiotherapy target segmentation, providing valuable insights toward clinically applicable automated radiotherapy planning systems. The benchmark is available at: https://hilab-git.github.io/SegRap2025_Challenge.
DINOv3-Guided Cross Fusion Framework for Semantic-aware CT generation from MRI and CBCT
Nov 15, 2025



Generating synthetic CT images from CBCT or MRI has a potential for efficient radiation dose planning and adaptive radiotherapy. However, existing CNN-based models lack global semantic understanding, while Transformers often overfit small medical datasets due to high model capacity and weak inductive bias. To address these limitations, we propose a DINOv3-Guided Cross Fusion (DGCF) framework that integrates a frozen self-supervised DINOv3 Transformer with a trainable CNN encoder-decoder. It hierarchically fuses global representation of Transformer and local features of CNN via a learnable cross fusion module, achieving balanced local appearance and contextual representation. Furthermore, we introduce a Multi-Level DINOv3 Perceptual (MLDP) loss that encourages semantic similarity between synthetic CT and the ground truth in DINOv3's feature space. Experiments on the SynthRAD2023 pelvic dataset demonstrate that DGCF achieved state-of-the-art performance in terms of MS-SSIM, PSNR and segmentation-based metrics on both MRI$\rightarrow$CT and CBCT$\rightarrow$CT translation tasks. To the best of our knowledge, this is the first work to employ DINOv3 representations for medical image translation, highlighting the potential of self-supervised Transformer guidance for semantic-aware CT synthesis. The code is available at https://github.com/HiLab-git/DGCF.
SRPL-SFDA: SAM-Guided Reliable Pseudo-Labels for Source-Free Domain Adaptation in Medical Image Segmentation
Jun 11, 2025Domain Adaptation (DA) is crucial for robust deployment of medical image segmentation models when applied to new clinical centers with significant domain shifts. Source-Free Domain Adaptation (SFDA) is appealing as it can deal with privacy concerns and access constraints on source-domain data during adaptation to target-domain data. However, SFDA faces challenges such as insufficient supervision in the target domain with unlabeled images. In this work, we propose a Segment Anything Model (SAM)-guided Reliable Pseudo-Labels method for SFDA (SRPL-SFDA) with three key components: 1) Test-Time Tri-branch Intensity Enhancement (T3IE) that not only improves quality of raw pseudo-labels in the target domain, but also leads to SAM-compatible inputs with three channels to better leverage SAM's zero-shot inference ability for refining the pseudo-labels; 2) A reliable pseudo-label selection module that rejects low-quality pseudo-labels based on Consistency of Multiple SAM Outputs (CMSO) under input perturbations with T3IE; and 3) A reliability-aware training procedure in the unlabeled target domain where reliable pseudo-labels are used for supervision and unreliable parts are regularized by entropy minimization. Experiments conducted on two multi-domain medical image segmentation datasets for fetal brain and the prostate respectively demonstrate that: 1) SRPL-SFDA effectively enhances pseudo-label quality in the unlabeled target domain, and improves SFDA performance by leveraging the reliability-aware training; 2) SRPL-SFDA outperformed state-of-the-art SFDA methods, and its performance is close to that of supervised training in the target domain. The code of this work is available online: https://github.com/HiLab-git/SRPL-SFDA.
SAM-aware Test-time Adaptation for Universal Medical Image Segmentation
Jun 05, 2025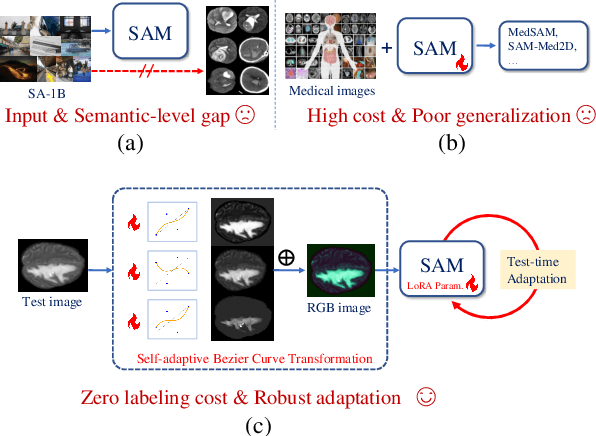
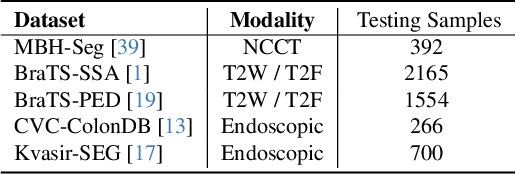
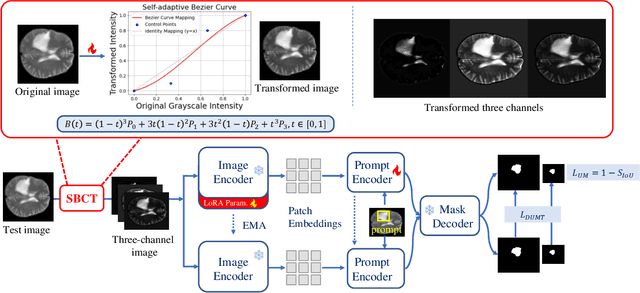
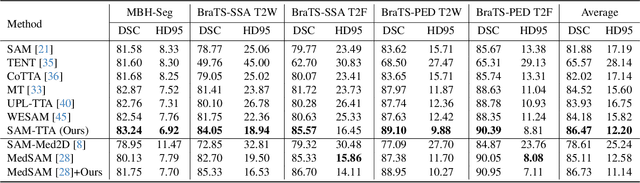
Universal medical image segmentation using the Segment Anything Model (SAM) remains challenging due to its limited adaptability to medical domains. Existing adaptations, such as MedSAM, enhance SAM's performance in medical imaging but at the cost of reduced generalization to unseen data. Therefore, in this paper, we propose SAM-aware Test-Time Adaptation (SAM-TTA), a fundamentally different pipeline that preserves the generalization of SAM while improving its segmentation performance in medical imaging via a test-time framework. SAM-TTA tackles two key challenges: (1) input-level discrepancies caused by differences in image acquisition between natural and medical images and (2) semantic-level discrepancies due to fundamental differences in object definition between natural and medical domains (e.g., clear boundaries vs. ambiguous structures). Specifically, our SAM-TTA framework comprises (1) Self-adaptive Bezier Curve-based Transformation (SBCT), which adaptively converts single-channel medical images into three-channel SAM-compatible inputs while maintaining structural integrity, to mitigate the input gap between medical and natural images, and (2) Dual-scale Uncertainty-driven Mean Teacher adaptation (DUMT), which employs consistency learning to align SAM's internal representations to medical semantics, enabling efficient adaptation without auxiliary supervision or expensive retraining. Extensive experiments on five public datasets demonstrate that our SAM-TTA outperforms existing TTA approaches and even surpasses fully fine-tuned models such as MedSAM in certain scenarios, establishing a new paradigm for universal medical image segmentation. Code can be found at https://github.com/JianghaoWu/SAM-TTA.
TAGS: A Test-Time Generalist-Specialist Framework with Retrieval-Augmented Reasoning and Verification
May 23, 2025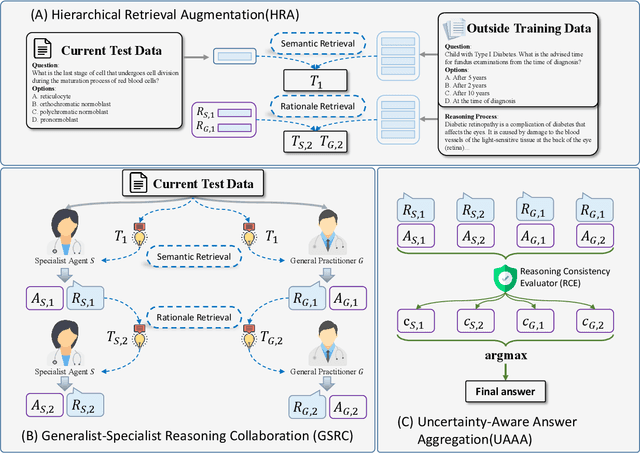
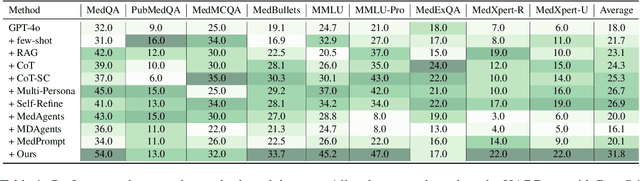
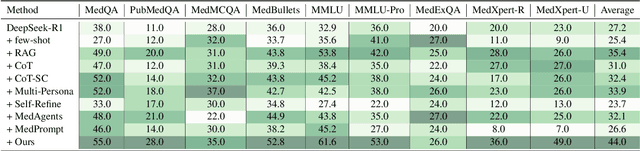
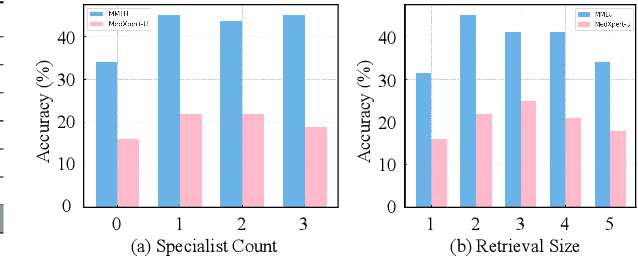
Recent advances such as Chain-of-Thought prompting have significantly improved large language models (LLMs) in zero-shot medical reasoning. However, prompting-based methods often remain shallow and unstable, while fine-tuned medical LLMs suffer from poor generalization under distribution shifts and limited adaptability to unseen clinical scenarios. To address these limitations, we present TAGS, a test-time framework that combines a broadly capable generalist with a domain-specific specialist to offer complementary perspectives without any model fine-tuning or parameter updates. To support this generalist-specialist reasoning process, we introduce two auxiliary modules: a hierarchical retrieval mechanism that provides multi-scale exemplars by selecting examples based on both semantic and rationale-level similarity, and a reliability scorer that evaluates reasoning consistency to guide final answer aggregation. TAGS achieves strong performance across nine MedQA benchmarks, boosting GPT-4o accuracy by 13.8%, DeepSeek-R1 by 16.8%, and improving a vanilla 7B model from 14.1% to 23.9%. These results surpass several fine-tuned medical LLMs, without any parameter updates. The code will be available at https://github.com/JianghaoWu/TAGS.
GLFC: Unified Global-Local Feature and Contrast Learning with Mamba-Enhanced UNet for Synthetic CT Generation from CBCT
Jan 06, 2025



Generating synthetic Computed Tomography (CT) images from Cone Beam Computed Tomography (CBCT) is desirable for improving the image quality of CBCT. Existing synthetic CT (sCT) generation methods using Convolutional Neural Networks (CNN) and Transformers often face difficulties in effectively capturing both global and local features and contrasts for high-quality sCT generation. In this work, we propose a Global-Local Feature and Contrast learning (GLFC) framework for sCT generation. First, a Mamba-Enhanced UNet (MEUNet) is introduced by integrating Mamba blocks into the skip connections of a high-resolution UNet for effective global and local feature learning. Second, we propose a Multiple Contrast Loss (MCL) that calculates synthetic loss at different intensity windows to improve quality for both soft tissues and bone regions. Experiments on the SynthRAD2023 dataset demonstrate that GLFC improved the SSIM of sCT from 77.91% to 91.50% compared with the original CBCT, and significantly outperformed several existing methods for sCT generation. The code is available at https://github.com/intelland/GLFC
FPL+: Filtered Pseudo Label-based Unsupervised Cross-Modality Adaptation for 3D Medical Image Segmentation
Apr 07, 2024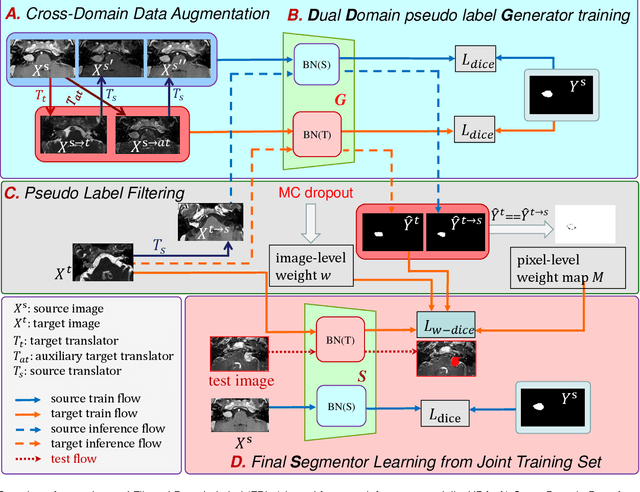
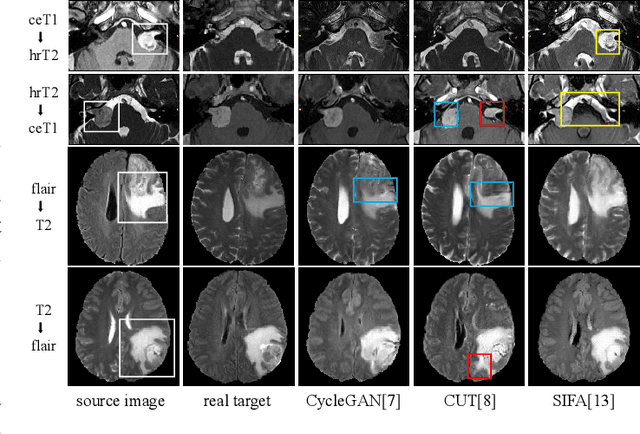
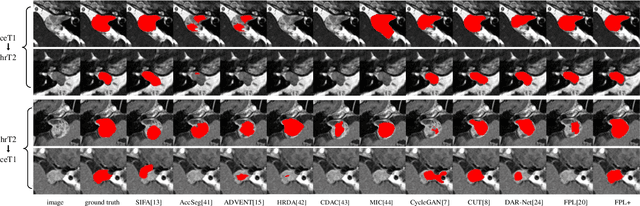

Adapting a medical image segmentation model to a new domain is important for improving its cross-domain transferability, and due to the expensive annotation process, Unsupervised Domain Adaptation (UDA) is appealing where only unlabeled images are needed for the adaptation. Existing UDA methods are mainly based on image or feature alignment with adversarial training for regularization, and they are limited by insufficient supervision in the target domain. In this paper, we propose an enhanced Filtered Pseudo Label (FPL+)-based UDA method for 3D medical image segmentation. It first uses cross-domain data augmentation to translate labeled images in the source domain to a dual-domain training set consisting of a pseudo source-domain set and a pseudo target-domain set. To leverage the dual-domain augmented images to train a pseudo label generator, domain-specific batch normalization layers are used to deal with the domain shift while learning the domain-invariant structure features, generating high-quality pseudo labels for target-domain images. We then combine labeled source-domain images and target-domain images with pseudo labels to train a final segmentor, where image-level weighting based on uncertainty estimation and pixel-level weighting based on dual-domain consensus are proposed to mitigate the adverse effect of noisy pseudo labels. Experiments on three public multi-modal datasets for Vestibular Schwannoma, brain tumor and whole heart segmentation show that our method surpassed ten state-of-the-art UDA methods, and it even achieved better results than fully supervised learning in the target domain in some cases.