 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeCapabilities of Gemini Models in Medicine
May 01, 2024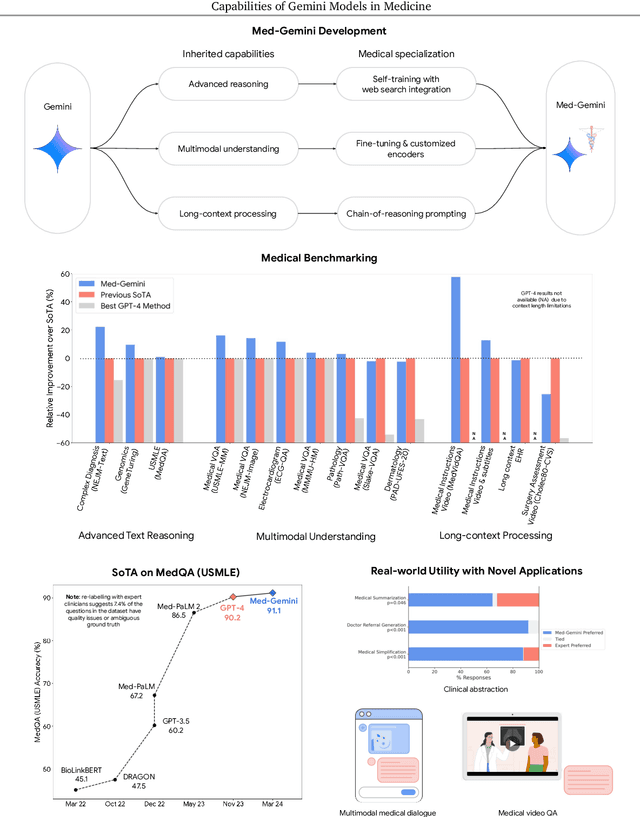
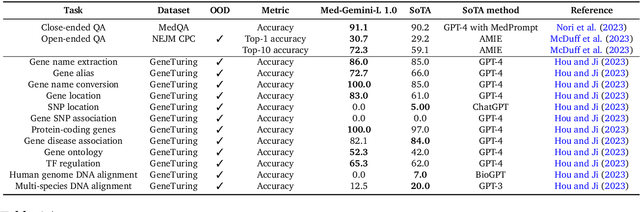
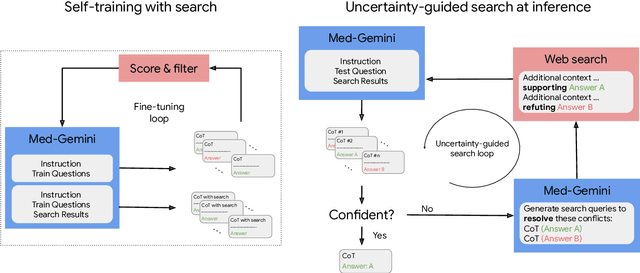
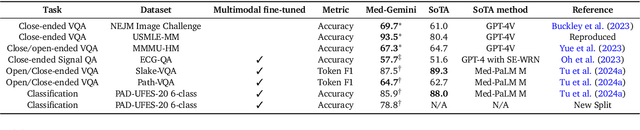
Excellence in a wide variety of medical applications poses considerable challenges for AI, requiring advanced reasoning, access to up-to-date medical knowledge and understanding of complex multimodal data. Gemini models, with strong general capabilities in multimodal and long-context reasoning, offer exciting possibilities in medicine. Building on these core strengths of Gemini, we introduce Med-Gemini, a family of highly capable multimodal models that are specialized in medicine with the ability to seamlessly use web search, and that can be efficiently tailored to novel modalities using custom encoders. We evaluate Med-Gemini on 14 medical benchmarks, establishing new state-of-the-art (SoTA) performance on 10 of them, and surpass the GPT-4 model family on every benchmark where a direct comparison is viable, often by a wide margin. On the popular MedQA (USMLE) benchmark, our best-performing Med-Gemini model achieves SoTA performance of 91.1% accuracy, using a novel uncertainty-guided search strategy. On 7 multimodal benchmarks including NEJM Image Challenges and MMMU (health & medicine), Med-Gemini improves over GPT-4V by an average relative margin of 44.5%. We demonstrate the effectiveness of Med-Gemini's long-context capabilities through SoTA performance on a needle-in-a-haystack retrieval task from long de-identified health records and medical video question answering, surpassing prior bespoke methods using only in-context learning. Finally, Med-Gemini's performance suggests real-world utility by surpassing human experts on tasks such as medical text summarization, alongside demonstrations of promising potential for multimodal medical dialogue, medical research and education. Taken together, our results offer compelling evidence for Med-Gemini's potential, although further rigorous evaluation will be crucial before real-world deployment in this safety-critical domain.
A Toolbox for Surfacing Health Equity Harms and Biases in Large Language Models
Mar 18, 2024Large language models (LLMs) hold immense promise to serve complex health information needs but also have the potential to introduce harm and exacerbate health disparities. Reliably evaluating equity-related model failures is a critical step toward developing systems that promote health equity. In this work, we present resources and methodologies for surfacing biases with potential to precipitate equity-related harms in long-form, LLM-generated answers to medical questions and then conduct an empirical case study with Med-PaLM 2, resulting in the largest human evaluation study in this area to date. Our contributions include a multifactorial framework for human assessment of LLM-generated answers for biases, and EquityMedQA, a collection of seven newly-released datasets comprising both manually-curated and LLM-generated questions enriched for adversarial queries. Both our human assessment framework and dataset design process are grounded in an iterative participatory approach and review of possible biases in Med-PaLM 2 answers to adversarial queries. Through our empirical study, we find that the use of a collection of datasets curated through a variety of methodologies, coupled with a thorough evaluation protocol that leverages multiple assessment rubric designs and diverse rater groups, surfaces biases that may be missed via narrower evaluation approaches. Our experience underscores the importance of using diverse assessment methodologies and involving raters of varying backgrounds and expertise. We emphasize that while our framework can identify specific forms of bias, it is not sufficient to holistically assess whether the deployment of an AI system promotes equitable health outcomes. We hope the broader community leverages and builds on these tools and methods towards realizing a shared goal of LLMs that promote accessible and equitable healthcare for all.
Augmentations vs Algorithms: What Works in Self-Supervised Learning
Mar 08, 2024



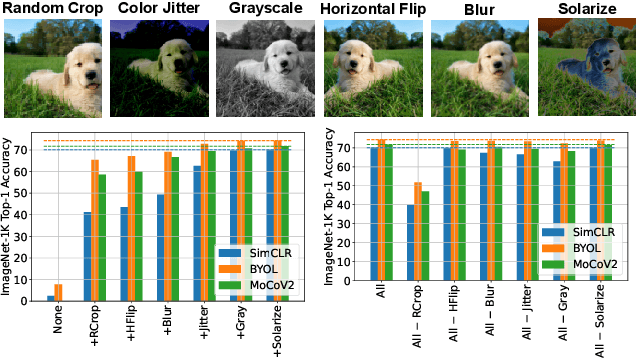
We study the relative effects of data augmentations, pretraining algorithms, and model architectures in Self-Supervised Learning (SSL). While the recent literature in this space leaves the impression that the pretraining algorithm is of critical importance to performance, understanding its effect is complicated by the difficulty in making objective and direct comparisons between methods. We propose a new framework which unifies many seemingly disparate SSL methods into a single shared template. Using this framework, we identify aspects in which methods differ and observe that in addition to changing the pretraining algorithm, many works also use new data augmentations or more powerful model architectures. We compare several popular SSL methods using our framework and find that many algorithmic additions, such as prediction networks or new losses, have a minor impact on downstream task performance (often less than $1\%$), while enhanced augmentation techniques offer more significant performance improvements ($2-4\%$). Our findings challenge the premise that SSL is being driven primarily by algorithmic improvements, and suggest instead a bitter lesson for SSL: that augmentation diversity and data / model scale are more critical contributors to recent advances in self-supervised learning.
Disentangling the Effects of Data Augmentation and Format Transform in Self-Supervised Learning of Image Representations
Dec 02, 2023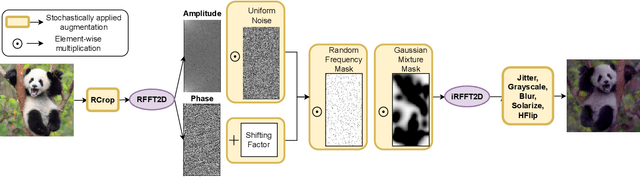
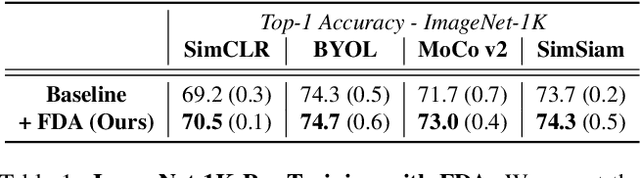
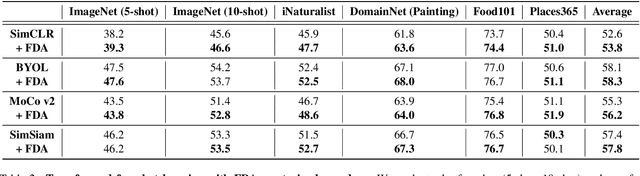
Self-Supervised Learning (SSL) enables training performant models using limited labeled data. One of the pillars underlying vision SSL is the use of data augmentations/perturbations of the input which do not significantly alter its semantic content. For audio and other temporal signals, augmentations are commonly used alongside format transforms such as Fourier transforms or wavelet transforms. Unlike augmentations, format transforms do not change the information contained in the data; rather, they express the same information in different coordinates. In this paper, we study the effects of format transforms and augmentations both separately and together on vision SSL. We define augmentations in frequency space called Fourier Domain Augmentations (FDA) and show that training SSL models on a combination of these and image augmentations can improve the downstream classification accuracy by up to 1.3% on ImageNet-1K. We also show improvements against SSL baselines in few-shot and transfer learning setups using FDA. Surprisingly, we also observe that format transforms can improve the quality of learned representations even without augmentations; however, the combination of the two techniques yields better quality.
Towards Generalist Biomedical AI
Jul 26, 2023



Medicine is inherently multimodal, with rich data modalities spanning text, imaging, genomics, and more. Generalist biomedical artificial intelligence (AI) systems that flexibly encode, integrate, and interpret this data at scale can potentially enable impactful applications ranging from scientific discovery to care delivery. To enable the development of these models, we first curate MultiMedBench, a new multimodal biomedical benchmark. MultiMedBench encompasses 14 diverse tasks such as medical question answering, mammography and dermatology image interpretation, radiology report generation and summarization, and genomic variant calling. We then introduce Med-PaLM Multimodal (Med-PaLM M), our proof of concept for a generalist biomedical AI system. Med-PaLM M is a large multimodal generative model that flexibly encodes and interprets biomedical data including clinical language, imaging, and genomics with the same set of model weights. Med-PaLM M reaches performance competitive with or exceeding the state of the art on all MultiMedBench tasks, often surpassing specialist models by a wide margin. We also report examples of zero-shot generalization to novel medical concepts and tasks, positive transfer learning across tasks, and emergent zero-shot medical reasoning. To further probe the capabilities and limitations of Med-PaLM M, we conduct a radiologist evaluation of model-generated (and human) chest X-ray reports and observe encouraging performance across model scales. In a side-by-side ranking on 246 retrospective chest X-rays, clinicians express a pairwise preference for Med-PaLM M reports over those produced by radiologists in up to 40.50% of cases, suggesting potential clinical utility. While considerable work is needed to validate these models in real-world use cases, our results represent a milestone towards the development of generalist biomedical AI systems.
Towards Expert-Level Medical Question Answering with Large Language Models
May 16, 2023



Recent artificial intelligence (AI) systems have reached milestones in "grand challenges" ranging from Go to protein-folding. The capability to retrieve medical knowledge, reason over it, and answer medical questions comparably to physicians has long been viewed as one such grand challenge. Large language models (LLMs) have catalyzed significant progress in medical question answering; Med-PaLM was the first model to exceed a "passing" score in US Medical Licensing Examination (USMLE) style questions with a score of 67.2% on the MedQA dataset. However, this and other prior work suggested significant room for improvement, especially when models' answers were compared to clinicians' answers. Here we present Med-PaLM 2, which bridges these gaps by leveraging a combination of base LLM improvements (PaLM 2), medical domain finetuning, and prompting strategies including a novel ensemble refinement approach. Med-PaLM 2 scored up to 86.5% on the MedQA dataset, improving upon Med-PaLM by over 19% and setting a new state-of-the-art. We also observed performance approaching or exceeding state-of-the-art across MedMCQA, PubMedQA, and MMLU clinical topics datasets. We performed detailed human evaluations on long-form questions along multiple axes relevant to clinical applications. In pairwise comparative ranking of 1066 consumer medical questions, physicians preferred Med-PaLM 2 answers to those produced by physicians on eight of nine axes pertaining to clinical utility (p < 0.001). We also observed significant improvements compared to Med-PaLM on every evaluation axis (p < 0.001) on newly introduced datasets of 240 long-form "adversarial" questions to probe LLM limitations. While further studies are necessary to validate the efficacy of these models in real-world settings, these results highlight rapid progress towards physician-level performance in medical question answering.
Large Language Models Encode Clinical Knowledge
Dec 26, 2022Large language models (LLMs) have demonstrated impressive capabilities in natural language understanding and generation, but the quality bar for medical and clinical applications is high. Today, attempts to assess models' clinical knowledge typically rely on automated evaluations on limited benchmarks. There is no standard to evaluate model predictions and reasoning across a breadth of tasks. To address this, we present MultiMedQA, a benchmark combining six existing open question answering datasets spanning professional medical exams, research, and consumer queries; and HealthSearchQA, a new free-response dataset of medical questions searched online. We propose a framework for human evaluation of model answers along multiple axes including factuality, precision, possible harm, and bias. In addition, we evaluate PaLM (a 540-billion parameter LLM) and its instruction-tuned variant, Flan-PaLM, on MultiMedQA. Using a combination of prompting strategies, Flan-PaLM achieves state-of-the-art accuracy on every MultiMedQA multiple-choice dataset (MedQA, MedMCQA, PubMedQA, MMLU clinical topics), including 67.6% accuracy on MedQA (US Medical License Exam questions), surpassing prior state-of-the-art by over 17%. However, human evaluation reveals key gaps in Flan-PaLM responses. To resolve this we introduce instruction prompt tuning, a parameter-efficient approach for aligning LLMs to new domains using a few exemplars. The resulting model, Med-PaLM, performs encouragingly, but remains inferior to clinicians. We show that comprehension, recall of knowledge, and medical reasoning improve with model scale and instruction prompt tuning, suggesting the potential utility of LLMs in medicine. Our human evaluations reveal important limitations of today's models, reinforcing the importance of both evaluation frameworks and method development in creating safe, helpful LLM models for clinical applications.
Contrastive Learning for Label-Efficient Semantic Segmentation
Dec 23, 2020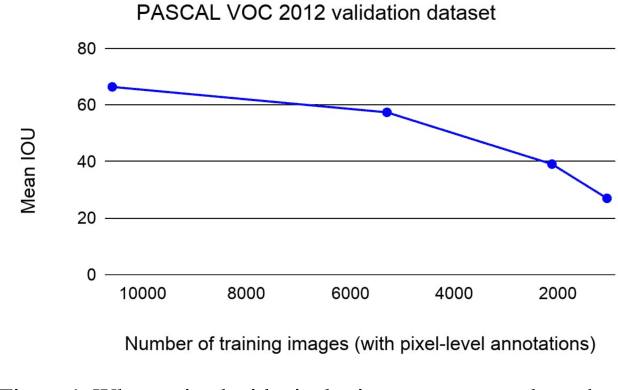
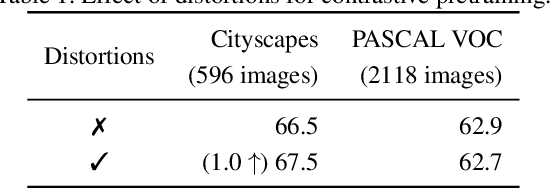
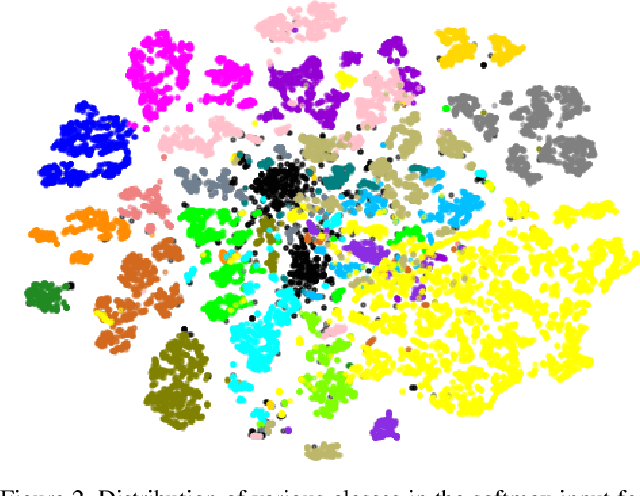
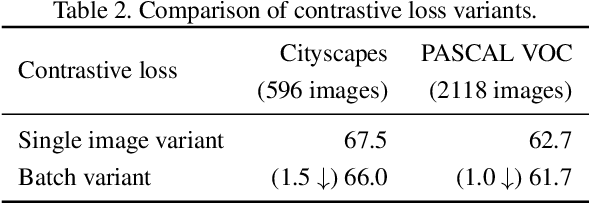
Collecting labeled data for the task of semantic segmentation is expensive and time-consuming, as it requires dense pixel-level annotations. While recent Convolutional Neural Network (CNN) based semantic segmentation approaches have achieved impressive results by using large amounts of labeled training data, their performance drops significantly as the amount of labeled data decreases. This happens because deep CNNs trained with the de facto cross-entropy loss can easily overfit to small amounts of labeled data. To address this issue, we propose a simple and effective contrastive learning-based training strategy in which we first pretrain the network using a pixel-wise class label-based contrastive loss, and then fine-tune it using the cross-entropy loss. This approach increases intra-class compactness and inter-class separability thereby resulting in a better pixel classifier. We demonstrate the effectiveness of the proposed training strategy in both fully-supervised and semi-supervised settings using the Cityscapes and PASCAL VOC 2012 segmentation datasets. Our results show that pretraining with label-based contrastive loss results in large performance gains (more than 20% absolute improvement in some settings) when the amount of labeled data is limited.