 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeOpen-H-Embodiment: A Large-Scale Dataset for Enabling Foundation Models in Medical Robotics
Apr 22, 2026Autonomous medical robots hold promise to improve patient outcomes, reduce provider workload, democratize access to care, and enable superhuman precision. However, autonomous medical robotics has been limited by a fundamental data problem: existing medical robotic datasets are small, single-embodiment, and rarely shared openly, restricting the development of foundation models that the field needs to advance. We introduce Open-H-Embodiment, the largest open dataset of medical robotic video with synchronized kinematics to date, spanning more than 49 institutions and multiple robotic platforms including the CMR Versius, Intuitive Surgical's da Vinci, da Vinci Research Kit (dVRK), Rob Surgical BiTrack, Virtual Incision's MIRA, Moon Surgical Maestro, and a variety of custom systems, spanning surgical manipulation, robotic ultrasound, and endoscopy procedures. We demonstrate the research enabled by this dataset through two foundation models. GR00T-H is the first open foundation vision-language-action model for medical robotics, which is the only evaluated model to achieve full end-to-end task completion on a structured suturing benchmark (25% of trials vs. 0% for all others) and achieves 64% average success across a 29-step ex vivo suturing sequence. We also train Cosmos-H-Surgical-Simulator, the first action-conditioned world model to enable multi-embodiment surgical simulation from a single checkpoint, spanning nine robotic platforms and supporting in silico policy evaluation and synthetic data generation for the medical domain. These results suggest that open, large-scale medical robot data collection can serve as critical infrastructure for the research community, enabling advances in robot learning, world modeling, and beyond.
SonoGym: High Performance Simulation for Challenging Surgical Tasks with Robotic Ultrasound
Jul 01, 2025Ultrasound (US) is a widely used medical imaging modality due to its real-time capabilities, non-invasive nature, and cost-effectiveness. Robotic ultrasound can further enhance its utility by reducing operator dependence and improving access to complex anatomical regions. For this, while deep reinforcement learning (DRL) and imitation learning (IL) have shown potential for autonomous navigation, their use in complex surgical tasks such as anatomy reconstruction and surgical guidance remains limited -- largely due to the lack of realistic and efficient simulation environments tailored to these tasks. We introduce SonoGym, a scalable simulation platform for complex robotic ultrasound tasks that enables parallel simulation across tens to hundreds of environments. Our framework supports realistic and real-time simulation of US data from CT-derived 3D models of the anatomy through both a physics-based and a generative modeling approach. Sonogym enables the training of DRL and recent IL agents (vision transformers and diffusion policies) for relevant tasks in robotic orthopedic surgery by integrating common robotic platforms and orthopedic end effectors. We further incorporate submodular DRL -- a recent method that handles history-dependent rewards -- for anatomy reconstruction and safe reinforcement learning for surgery. Our results demonstrate successful policy learning across a range of scenarios, while also highlighting the limitations of current methods in clinically relevant environments. We believe our simulation can facilitate research in robot learning approaches for such challenging robotic surgery applications. Dataset, codes, and videos are publicly available at https://sonogym.github.io/.
Acquiring Submillimeter-Accurate Multi-Task Vision Datasets for Computer-Assisted Orthopedic Surgery
Jan 26, 2025Advances in computer vision, particularly in optical image-based 3D reconstruction and feature matching, enable applications like marker-less surgical navigation and digitization of surgery. However, their development is hindered by a lack of suitable datasets with 3D ground truth. This work explores an approach to generating realistic and accurate ex vivo datasets tailored for 3D reconstruction and feature matching in open orthopedic surgery. A set of posed images and an accurately registered ground truth surface mesh of the scene are required to develop vision-based 3D reconstruction and matching methods suitable for surgery. We propose a framework consisting of three core steps and compare different methods for each step: 3D scanning, calibration of viewpoints for a set of high-resolution RGB images, and an optical-based method for scene registration. We evaluate each step of this framework on an ex vivo scoliosis surgery using a pig spine, conducted under real operating room conditions. A mean 3D Euclidean error of 0.35 mm is achieved with respect to the 3D ground truth. The proposed method results in submillimeter accurate 3D ground truths and surgical images with a spatial resolution of 0.1 mm. This opens the door to acquiring future surgical datasets for high-precision applications.
SurgPointTransformer: Vertebrae Shape Completion with RGB-D Data
Oct 02, 2024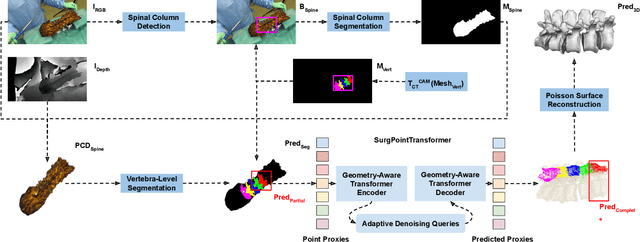
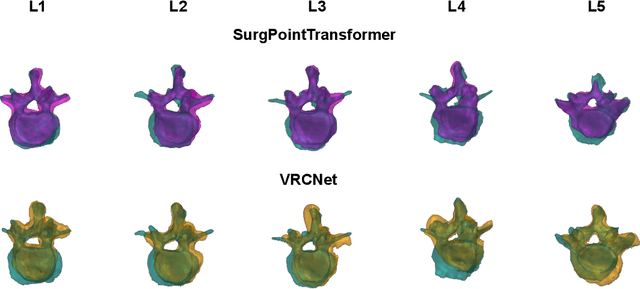
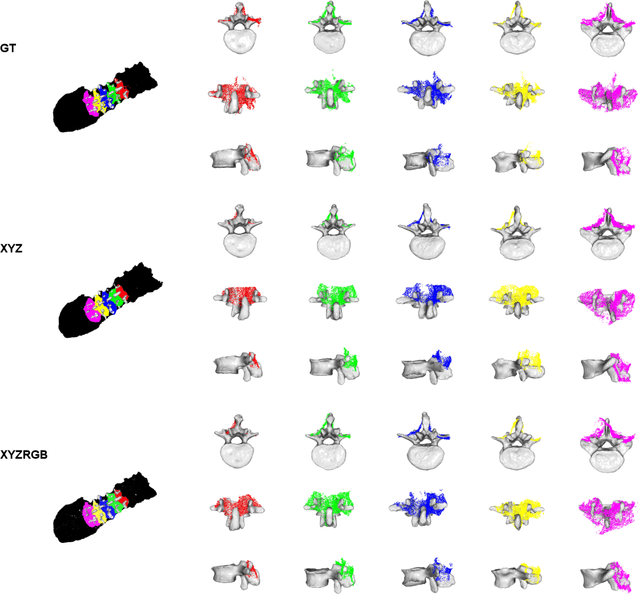
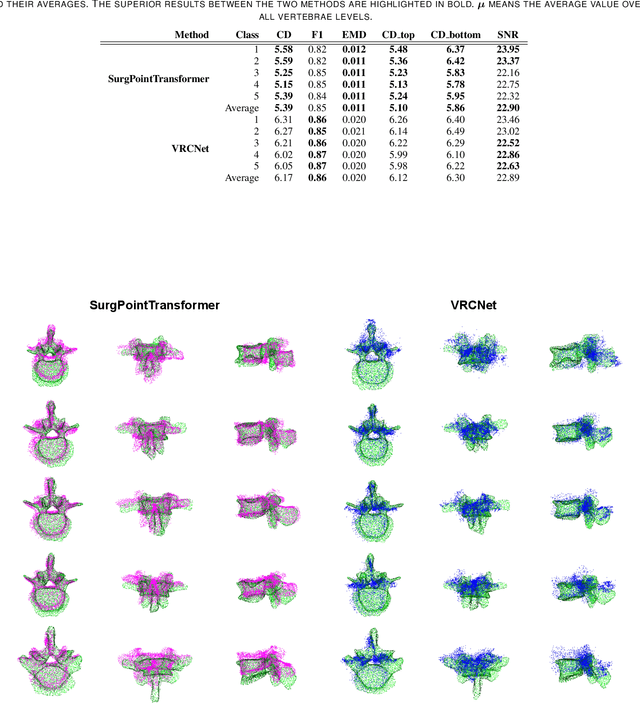
State-of-the-art computer- and robot-assisted surgery systems heavily depend on intraoperative imaging technologies such as CT and fluoroscopy to generate detailed 3D visualization of the patient's anatomy. While imaging techniques are highly accurate, they are based on ionizing radiation and expose patients and clinicians. This study introduces an alternative, radiation-free approach for reconstructing the 3D spine anatomy using RGB-D data. Drawing inspiration from the 3D "mental map" that surgeons form during surgeries, we introduce SurgPointTransformer, a shape completion approach for surgical applications that can accurately reconstruct the unexposed spine regions from sparse observations of the exposed surface. Our method involves two main steps: segmentation and shape completion. The segmentation step includes spinal column localization and segmentation, followed by vertebra-wise segmentation. The segmented vertebra point clouds are then subjected to SurgPointTransformer, which leverages an attention mechanism to learn patterns between visible surface features and the underlying anatomy. For evaluation, we utilize an ex-vivo dataset of nine specimens. Their CT data is used to establish ground truth data that were used to compare to the outputs of our methods. Our method significantly outperforms the state-of-the-art baselines, achieving an average Chamfer Distance of 5.39, an F-Score of 0.85, an Earth Mover's Distance of 0.011, and a Signal-to-Noise Ratio of 22.90 dB. This study demonstrates the potential of our reconstruction method for 3D vertebral shape completion. It enables 3D reconstruction of the entire lumbar spine and surgical guidance without ionizing radiation or invasive imaging. Our work contributes to computer-aided and robot-assisted surgery, advancing the perception and intelligence of these systems.
Creating a Digital Twin of Spinal Surgery: A Proof of Concept
Mar 25, 2024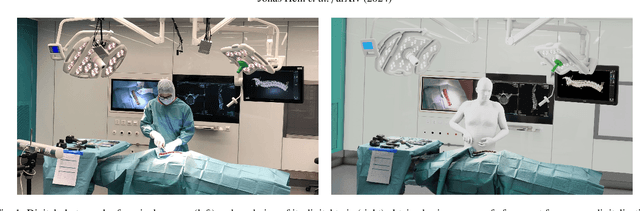
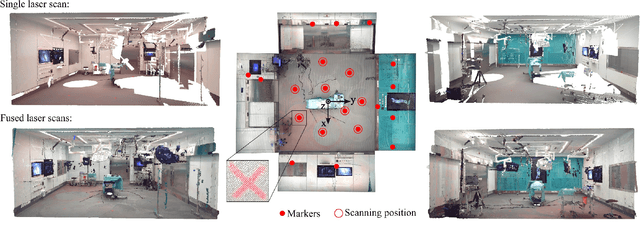
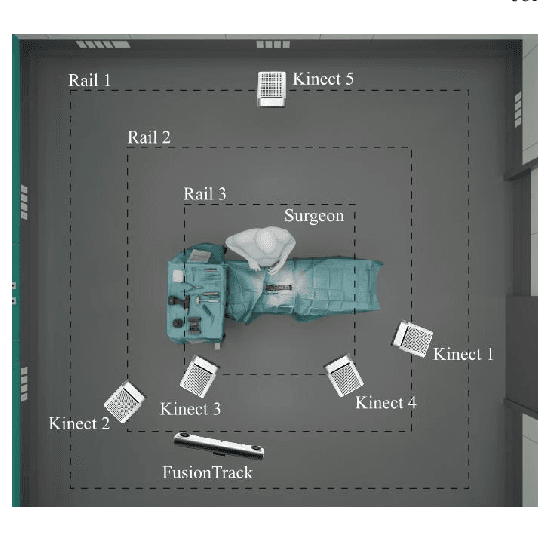
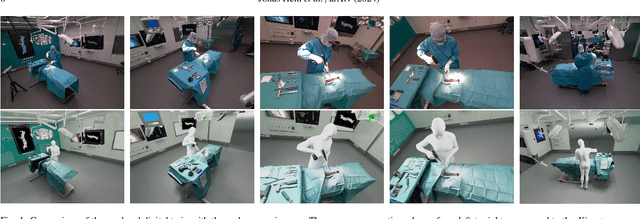
Surgery digitalization is the process of creating a virtual replica of real-world surgery, also referred to as a surgical digital twin (SDT). It has significant applications in various fields such as education and training, surgical planning, and automation of surgical tasks. Given their detailed representations of surgical procedures, SDTs are an ideal foundation for machine learning methods, enabling automatic generation of training data. In robotic surgery, SDTs can provide realistic virtual environments in which robots may learn through trial and error. In this paper, we present a proof of concept (PoC) for surgery digitalization that is applied to an ex-vivo spinal surgery performed in realistic conditions. The proposed digitalization focuses on the acquisition and modelling of the geometry and appearance of the entire surgical scene. We employ five RGB-D cameras for dynamic 3D reconstruction of the surgeon, a high-end camera for 3D reconstruction of the anatomy, an infrared stereo camera for surgical instrument tracking, and a laser scanner for 3D reconstruction of the operating room and data fusion. We justify the proposed methodology, discuss the challenges faced and further extensions of our prototype. While our PoC partially relies on manual data curation, its high quality and great potential motivate the development of automated methods for the creation of SDTs. The quality of our SDT can be assessed in a rendered video available at https://youtu.be/LqVaWGgaTMY .
Safe Deep RL for Intraoperative Planning of Pedicle Screw Placement
May 10, 2023



Spinal fusion surgery requires highly accurate implantation of pedicle screw implants, which must be conducted in critical proximity to vital structures with a limited view of anatomy. Robotic surgery systems have been proposed to improve placement accuracy, however, state-of-the-art systems suffer from the limitations of open-loop approaches, as they follow traditional concepts of preoperative planning and intraoperative registration, without real-time recalculation of the surgical plan. In this paper, we propose an intraoperative planning approach for robotic spine surgery that leverages real-time observation for drill path planning based on Safe Deep Reinforcement Learning (DRL). The main contributions of our method are (1) the capability to guarantee safe actions by introducing an uncertainty-aware distance-based safety filter; and (2) the ability to compensate for incomplete intraoperative anatomical information, by encoding a-priori knowledge about anatomical structures with a network pre-trained on high-fidelity anatomical models. Planning quality was assessed by quantitative comparison with the gold standard (GS) drill planning. In experiments with 5 models derived from real magnetic resonance imaging (MRI) data, our approach was capable of achieving 90% bone penetration with respect to the GS while satisfying safety requirements, even under observation and motion uncertainty. To the best of our knowledge, our approach is the first safe DRL approach focusing on orthopedic surgeries.
Next-generation Surgical Navigation: Multi-view Marker-less 6DoF Pose Estimation of Surgical Instruments
May 05, 2023



State-of-the-art research of traditional computer vision is increasingly leveraged in the surgical domain. A particular focus in computer-assisted surgery is to replace marker-based tracking systems for instrument localization with pure image-based 6DoF pose estimation. However, the state of the art has not yet met the accuracy required for surgical navigation. In this context, we propose a high-fidelity marker-less optical tracking system for surgical instrument localization. We developed a multi-view camera setup consisting of static and mobile cameras and collected a large-scale RGB-D video dataset with dedicated synchronization and data fusions methods. Different state-of-the-art pose estimation methods were integrated into a deep learning pipeline and evaluated on multiple camera configurations. Furthermore, the performance impacts of different input modalities and camera positions, as well as training on purely synthetic data, were compared. The best model achieved an average position and orientation error of 1.3 mm and 1.0{\deg} for a surgical drill as well as 3.8 mm and 5.2{\deg} for a screwdriver. These results significantly outperform related methods in the literature and are close to clinical-grade accuracy, demonstrating that marker-less tracking of surgical instruments is becoming a feasible alternative to existing marker-based systems.
Automatic breach detection during spine pedicle drilling based on vibroacoustic sensing
Mar 27, 2023



Pedicle drilling is a complex and critical spinal surgery task. Detecting breach or penetration of the surgical tool to the cortical wall during pilot-hole drilling is essential to avoid damage to vital anatomical structures adjacent to the pedicle, such as the spinal cord, blood vessels, and nerves. Currently, the guidance of pedicle drilling is done using image-guided methods that are radiation intensive and limited to the preoperative information. This work proposes a new radiation-free breach detection algorithm leveraging a non-visual sensor setup in combination with deep learning approach. Multiple vibroacoustic sensors, such as a contact microphone, a free-field microphone, a tri-axial accelerometer, a uni-axial accelerometer, and an optical tracking system were integrated into the setup. Data were collected on four cadaveric human spines, ranging from L5 to T10. An experienced spine surgeon drilled the pedicles relying on optical navigation. A new automatic labeling method based on the tracking data was introduced. Labeled data was subsequently fed to the network in mel-spectrograms, classifying the data into breach and non-breach. Different sensor types, sensor positioning, and their combinations were evaluated. The best results in breach recall for individual sensors could be achieved using contact microphones attached to the dorsal skin (85.8\%) and uni-axial accelerometers clamped to the spinous process of the drilled vertebra (81.0\%). The best-performing data fusion model combined the latter two sensors with a breach recall of 98\%. The proposed method shows the great potential of non-visual sensor fusion for avoiding screw misplacement and accidental bone breaches during pedicle drilling and could be extended to further surgical applications.