 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeStraightTrack: Towards Mixed Reality Navigation System for Percutaneous K-wire Insertion
Oct 02, 2024



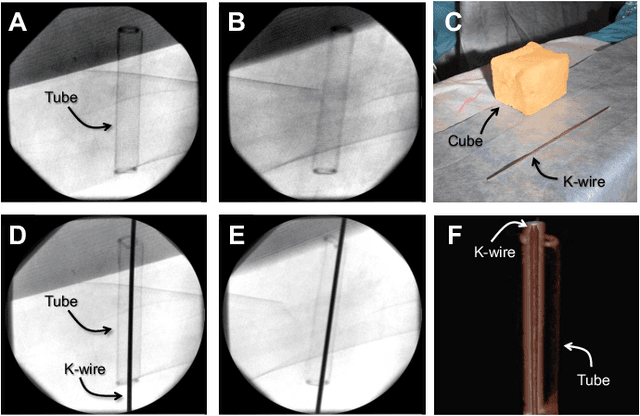
In percutaneous pelvic trauma surgery, accurate placement of Kirschner wires (K-wires) is crucial to ensure effective fracture fixation and avoid complications due to breaching the cortical bone along an unsuitable trajectory. Surgical navigation via mixed reality (MR) can help achieve precise wire placement in a low-profile form factor. Current approaches in this domain are as yet unsuitable for real-world deployment because they fall short of guaranteeing accurate visual feedback due to uncontrolled bending of the wire. To ensure accurate feedback, we introduce StraightTrack, an MR navigation system designed for percutaneous wire placement in complex anatomy. StraightTrack features a marker body equipped with a rigid access cannula that mitigates wire bending due to interactions with soft tissue and a covered bony surface. Integrated with an Optical See-Through Head-Mounted Display (OST HMD) capable of tracking the cannula body, StraightTrack offers real-time 3D visualization and guidance without external trackers, which are prone to losing line-of-sight. In phantom experiments with two experienced orthopedic surgeons, StraightTrack improves wire placement accuracy, achieving the ideal trajectory within $5.26 \pm 2.29$ mm and $2.88 \pm 1.49$ degree, compared to over 12.08 mm and 4.07 degree for comparable methods. As MR navigation systems continue to mature, StraightTrack realizes their potential for internal fracture fixation and other percutaneous orthopedic procedures.
FluoroSAM: A Language-aligned Foundation Model for X-ray Image Segmentation
Mar 12, 2024Automated X-ray image segmentation would accelerate research and development in diagnostic and interventional precision medicine. Prior efforts have contributed task-specific models capable of solving specific image analysis problems, but the utility of these models is restricted to their particular task domain, and expanding to broader use requires additional data, labels, and retraining efforts. Recently, foundation models (FMs) -- machine learning models trained on large amounts of highly variable data thus enabling broad applicability -- have emerged as promising tools for automated image analysis. Existing FMs for medical image analysis focus on scenarios and modalities where objects are clearly defined by visually apparent boundaries, such as surgical tool segmentation in endoscopy. X-ray imaging, by contrast, does not generally offer such clearly delineated boundaries or structure priors. During X-ray image formation, complex 3D structures are projected in transmission onto the imaging plane, resulting in overlapping features of varying opacity and shape. To pave the way toward an FM for comprehensive and automated analysis of arbitrary medical X-ray images, we develop FluoroSAM, a language-aligned variant of the Segment-Anything Model, trained from scratch on 1.6M synthetic X-ray images. FluoroSAM is trained on data including masks for 128 organ types and 464 non-anatomical objects, such as tools and implants. In real X-ray images of cadaveric specimens, FluoroSAM is able to segment bony anatomical structures based on text-only prompting with 0.51 and 0.79 DICE with point-based refinement, outperforming competing SAM variants for all structures. FluoroSAM is also capable of zero-shot generalization to segmenting classes beyond the training set thanks to its language alignment, which we demonstrate for full lung segmentation on real chest X-rays.
Pelphix: Surgical Phase Recognition from X-ray Images in Percutaneous Pelvic Fixation
Apr 18, 2023


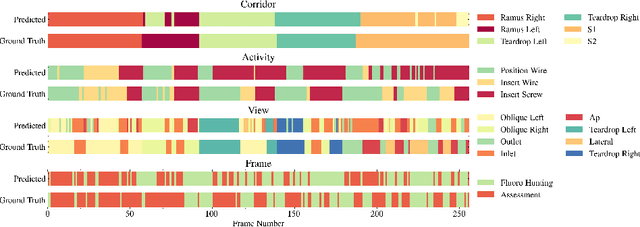
Surgical phase recognition (SPR) is a crucial element in the digital transformation of the modern operating theater. While SPR based on video sources is well-established, incorporation of interventional X-ray sequences has not yet been explored. This paper presents Pelphix, a first approach to SPR for X-ray-guided percutaneous pelvic fracture fixation, which models the procedure at four levels of granularity -- corridor, activity, view, and frame value -- simulating the pelvic fracture fixation workflow as a Markov process to provide fully annotated training data. Using added supervision from detection of bony corridors, tools, and anatomy, we learn image representations that are fed into a transformer model to regress surgical phases at the four granularity levels. Our approach demonstrates the feasibility of X-ray-based SPR, achieving an average accuracy of 93.8% on simulated sequences and 67.57% in cadaver across all granularity levels, with up to 88% accuracy for the target corridor in real data. This work constitutes the first step toward SPR for the X-ray domain, establishing an approach to categorizing phases in X-ray-guided surgery, simulating realistic image sequences to enable machine learning model development, and demonstrating that this approach is feasible for the analysis of real procedures. As X-ray-based SPR continues to mature, it will benefit procedures in orthopedic surgery, angiography, and interventional radiology by equipping intelligent surgical systems with situational awareness in the operating room.
Exploring Partial Intrinsic and Extrinsic Symmetry in 3D Medical Imaging
Mar 04, 2020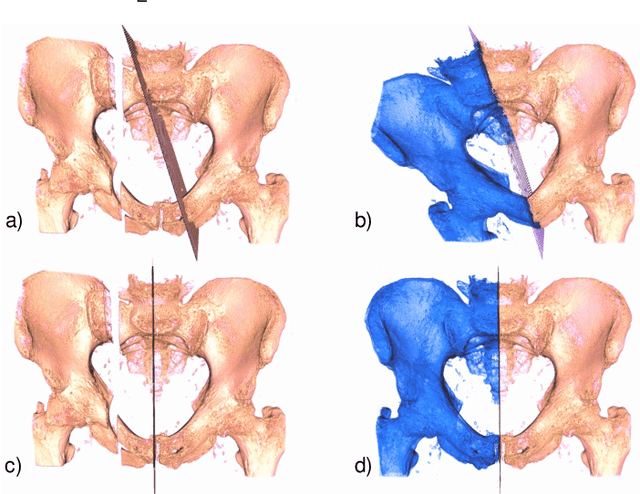

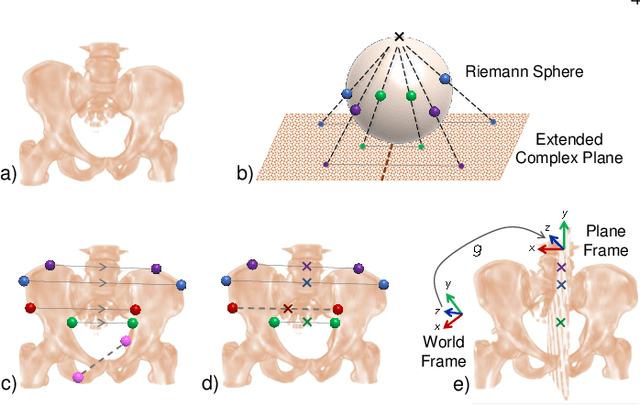

We present a novel methodology to detect imperfect bilateral symmetry in CT of human anatomy. In this paper, the structurally symmetric nature of the pelvic bone is explored and is used to provide interventional image augmentation for treatment of unilateral fractures in patients with traumatic injuries. The mathematical basis of our solution is on the incorporation of attributes and characteristics that satisfy the properties of intrinsic and extrinsic symmetry and are robust to outliers. In the first step, feature points that satisfy intrinsic symmetry are automatically detected in the M\"obius space defined on the CT data. These features are then pruned via a two-stage RANSAC to attain correspondences that satisfy also the extrinsic symmetry. Then, a disparity function based on Tukey's biweight robust estimator is introduced and minimized to identify a symmetry plane parametrization that yields maximum contralateral similarity. Finally, a novel regularization term is introduced to enhance similarity between bone density histograms across the partial symmetry plane, relying on the important biological observation that, even if injured, the dislocated bone segments remain within the body. Our extensive evaluations on various cases of common fracture types demonstrate the validity of the novel concepts and the robustness and accuracy of the proposed method.
Spatiotemporal-Aware Augmented Reality: Redefining HCI in Image-Guided Therapy
Mar 04, 2020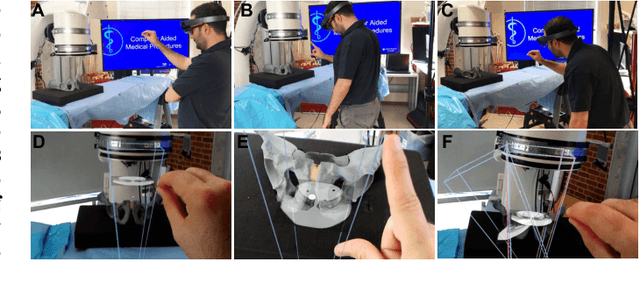
Suboptimal interaction with patient data and challenges in mastering 3D anatomy based on ill-posed 2D interventional images are essential concerns in image-guided therapies. Augmented reality (AR) has been introduced in the operating rooms in the last decade; however, in image-guided interventions, it has often only been considered as a visualization device improving traditional workflows. As a consequence, the technology is gaining minimum maturity that it requires to redefine new procedures, user interfaces, and interactions. The main contribution of this paper is to reveal how exemplary workflows are redefined by taking full advantage of head-mounted displays when entirely co-registered with the imaging system at all times. The proposed AR landscape is enabled by co-localizing the users and the imaging devices via the operating room environment and exploiting all involved frustums to move spatial information between different bodies. The awareness of the system from the geometric and physical characteristics of X-ray imaging allows the redefinition of different human-machine interfaces. We demonstrate that this AR paradigm is generic, and can benefit a wide variety of procedures. Our system achieved an error of $4.76\pm2.91$ mm for placing K-wire in a fracture management procedure, and yielded errors of $1.57\pm1.16^\circ$ and $1.46\pm1.00^\circ$ in the abduction and anteversion angles, respectively, for total hip arthroplasty. We hope that our holistic approach towards improving the interface of surgery not only augments the surgeon's capabilities but also augments the surgical team's experience in carrying out an effective intervention with reduced complications and provide novel approaches of documenting procedures for training purposes.
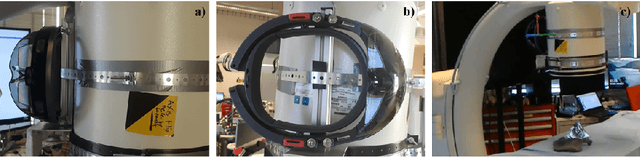
Augmented Reality-based Feedback for Technician-in-the-loop C-arm Repositioning
Jun 22, 2018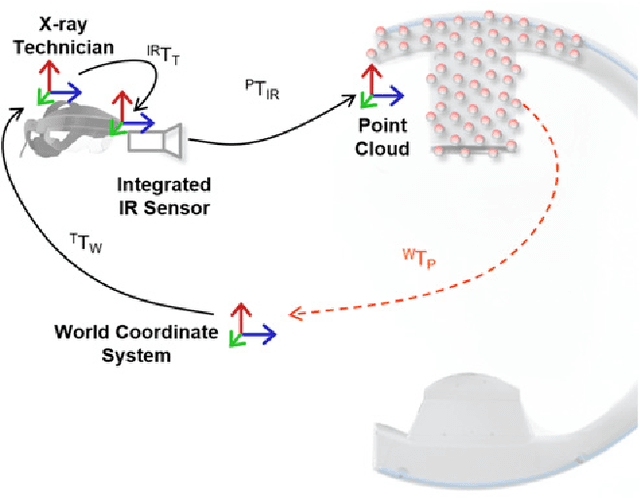
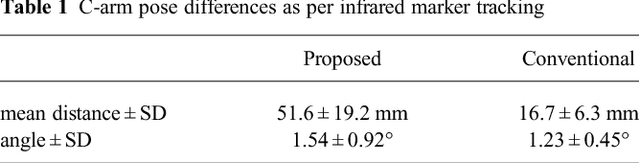


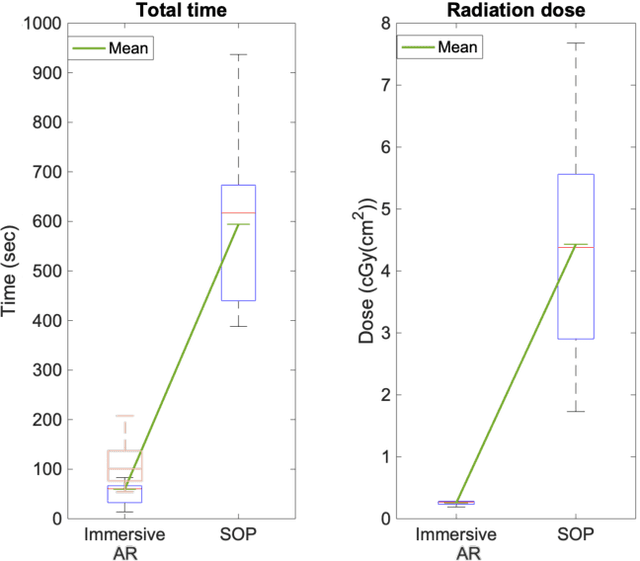
Interventional C-arm imaging is crucial to percutaneous orthopedic procedures as it enables the surgeon to monitor the progress of surgery on the anatomy level. Minimally invasive interventions require repeated acquisition of X-ray images from different anatomical views to verify tool placement. Achieving and reproducing these views often comes at the cost of increased surgical time and radiation dose to both patient and staff. This work proposes a marker-free "technician-in-the-loop" Augmented Reality (AR) solution for C-arm repositioning. The X-ray technician operating the C-arm interventionally is equipped with a head-mounted display capable of recording desired C-arm poses in 3D via an integrated infrared sensor. For C-arm repositioning to a particular target view, the recorded C-arm pose is restored as a virtual object and visualized in an AR environment, serving as a perceptual reference for the technician. We conduct experiments in a setting simulating orthopedic trauma surgery. Our proof-of-principle findings indicate that the proposed system can decrease the 2.76 X-ray images required per desired view down to zero, suggesting substantial reductions of radiation dose during C-arm repositioning. The proposed AR solution is a first step towards facilitating communication between the surgeon and the surgical staff, improving the quality of surgical image acquisition, and enabling context-aware guidance for surgery rooms of the future. The concept of technician-in-the-loop design will become relevant to various interventions considering the expected advancements of sensing and wearable computing in the near future.
Closing the Calibration Loop: An Inside-out-tracking Paradigm for Augmented Reality in Orthopedic Surgery
Mar 22, 2018

In percutaneous orthopedic interventions the surgeon attempts to reduce and fixate fractures in bony structures. The complexity of these interventions arises when the surgeon performs the challenging task of navigating surgical tools percutaneously only under the guidance of 2D interventional X-ray imaging. Moreover, the intra-operatively acquired data is only visualized indirectly on external displays. In this work, we propose a flexible Augmented Reality (AR) paradigm using optical see-through head mounted displays. The key technical contribution of this work includes the marker-less and dynamic tracking concept which closes the calibration loop between patient, C-arm and the surgeon. This calibration is enabled using Simultaneous Localization and Mapping of the environment of the operating theater. In return, the proposed solution provides in situ visualization of pre- and intra-operative 3D medical data directly at the surgical site. We demonstrate pre-clinical evaluation of a prototype system, and report errors for calibration and target registration. Finally, we demonstrate the usefulness of the proposed inside-out tracking system in achieving "bull's eye" view for C-arm-guided punctures. This AR solution provides an intuitive visualization of the anatomy and can simplify the hand-eye coordination for the orthopedic surgeon.
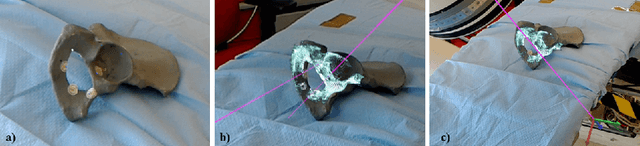
X-ray-transform Invariant Anatomical Landmark Detection for Pelvic Trauma Surgery
Mar 22, 2018

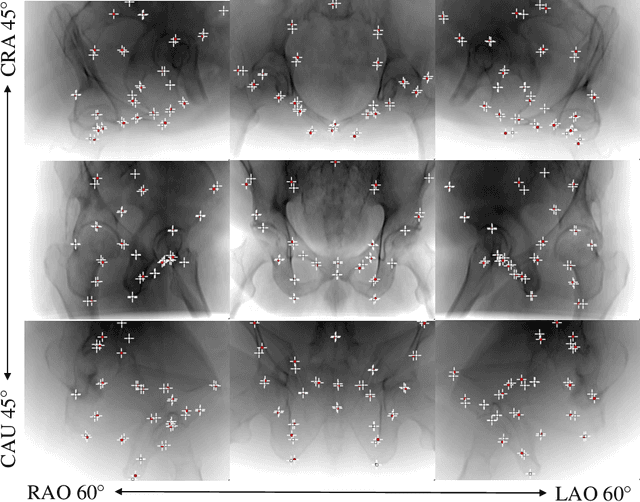
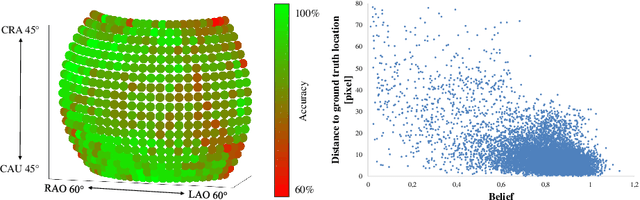
X-ray image guidance enables percutaneous alternatives to complex procedures. Unfortunately, the indirect view onto the anatomy in addition to projective simplification substantially increase the task-load for the surgeon. Additional 3D information such as knowledge of anatomical landmarks can benefit surgical decision making in complicated scenarios. Automatic detection of these landmarks in transmission imaging is challenging since image-domain features characteristic to a certain landmark change substantially depending on the viewing direction. Consequently and to the best of our knowledge, the above problem has not yet been addressed. In this work, we present a method to automatically detect anatomical landmarks in X-ray images independent of the viewing direction. To this end, a sequential prediction framework based on convolutional layers is trained on synthetically generated data of the pelvic anatomy to predict 23 landmarks in single X-ray images. View independence is contingent on training conditions and, here, is achieved on a spherical segment covering (120 x 90) degrees in LAO/RAO and CRAN/CAUD, respectively, centered around AP. On synthetic data, the proposed approach achieves a mean prediction error of 5.6 +- 4.5 mm. We demonstrate that the proposed network is immediately applicable to clinically acquired data of the pelvis. In particular, we show that our intra-operative landmark detection together with pre-operative CT enables X-ray pose estimation which, ultimately, benefits initialization of image-based 2D/3D registration.
On-the-fly Augmented Reality for Orthopaedic Surgery Using a Multi-Modal Fiducial
Jan 04, 2018Fluoroscopic X-ray guidance is a cornerstone for percutaneous orthopaedic surgical procedures. However, two-dimensional observations of the three-dimensional anatomy suffer from the effects of projective simplification. Consequently, many X-ray images from various orientations need to be acquired for the surgeon to accurately assess the spatial relations between the patient's anatomy and the surgical tools. In this paper, we present an on-the-fly surgical support system that provides guidance using augmented reality and can be used in quasi-unprepared operating rooms. The proposed system builds upon a multi-modality marker and simultaneous localization and mapping technique to co-calibrate an optical see-through head mounted display to a C-arm fluoroscopy system. Then, annotations on the 2D X-ray images can be rendered as virtual objects in 3D providing surgical guidance. We quantitatively evaluate the components of the proposed system, and finally, design a feasibility study on a semi-anthropomorphic phantom. The accuracy of our system was comparable to the traditional image-guided technique while substantially reducing the number of acquired X-ray images as well as procedure time. Our promising results encourage further research on the interaction between virtual and real objects, that we believe will directly benefit the proposed method. Further, we would like to explore the capabilities of our on-the-fly augmented reality support system in a larger study directed towards common orthopaedic interventions.
* S. Andress, A. Johnson, M. Unberath, and A. Winkler have contributed equally and are listed in alphabetical order
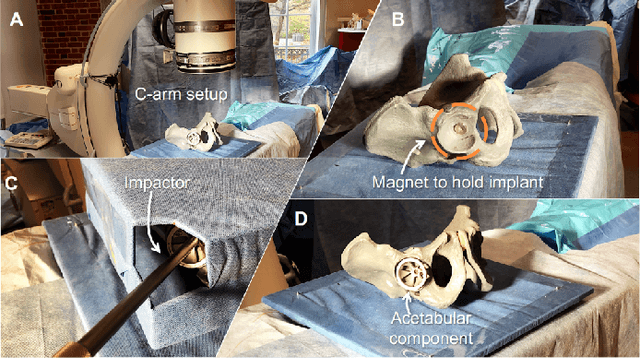
Plan in 2D, execute in 3D: An augmented reality solution for cup placement in total hip arthroplasty
Jan 04, 2018Reproducibly achieving proper implant alignment is a critical step in total hip arthroplasty (THA) procedures that has been shown to substantially affect patient outcome. In current practice, correct alignment of the acetabular cup is verified in C-arm X-ray images that are acquired in an anterior-posterior (AP) view. Favorable surgical outcome is, therefore, heavily dependent on the surgeon's experience in understanding the 3D orientation of a hemispheric implant from 2D AP projection images. This work proposes an easy to use intra-operative component planning system based on two C-arm X-ray images that is combined with 3D augmented reality (AR) visualization that simplifies impactor and cup placement according to the planning by providing a real-time RGBD data overlay. We evaluate the feasibility of our system in a user study comprising four orthopedic surgeons at the Johns Hopkins Hospital, and also report errors in translation, anteversion, and abduction as low as 1.98 mm, 1.10 degrees, and 0.53 degrees, respectively. The promising performance of this AR solution shows that deploying this system could eliminate the need for excessive radiation, simplify the intervention, and enable reproducibly accurate placement of acetabular implants.