 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeLeveraging Support Vector Regression for Outcome Prediction in Personalized Ultra-fractionated Stereotactic Adaptive Radiotherapy
Sep 09, 2025Personalized ultra-fractionated stereotactic adaptive radiotherapy (PULSAR) is a novel treatment that delivers radiation in pulses of protracted intervals. Accurate prediction of gross tumor volume (GTV) changes through regression models has substantial prognostic value. This study aims to develop a multi-omics based support vector regression (SVR) model for predicting GTV change. A retrospective cohort of 39 patients with 69 brain metastases was analyzed, based on radiomics (MRI images) and dosiomics (dose maps) features. Delta features were computed to capture relative changes between two time points. A feature selection pipeline using least absolute shrinkage and selection operator (Lasso) algorithm with weight- or frequency-based ranking criterion was implemented. SVR models with various kernels were evaluated using the coefficient of determination (R2) and relative root mean square error (RRMSE). Five-fold cross-validation with 10 repeats was employed to mitigate the limitation of small data size. Multi-omics models that integrate radiomics, dosiomics, and their delta counterparts outperform individual-omics models. Delta-radiomic features play a critical role in enhancing prediction accuracy relative to features at single time points. The top-performing model achieves an R2 of 0.743 and an RRMSE of 0.022. The proposed multi-omics SVR model shows promising performance in predicting continuous change of GTV. It provides a more quantitative and personalized approach to assist patient selection and treatment adjustment in PULSAR.
Exploring Strategies for Personalized Radiation Therapy: Part III Identifying genetic determinants for Radiation Response with Meta Learning
Aug 11, 2025



Radiation response in cancer is shaped by complex, patient specific biology, yet current treatment strategies often rely on uniform dose prescriptions without accounting for tumor heterogeneity. In this study, we introduce a meta learning framework for one-shot prediction of radiosensitivity measured by SF2 using cell line level gene expression data. Unlike the widely used Radiosensitivity Index RSI a rank-based linear model trained on a fixed 10-gene signature, our proposed meta-learned model allows the importance of each gene to vary by sample through fine tuning. This flexibility addresses key limitations of static models like RSI, which assume uniform gene contributions across tumor types and discard expression magnitude and gene gene interactions. Our results show that meta learning offers robust generalization to unseen samples and performs well in tumor subgroups with high radiosensitivity variability, such as adenocarcinoma and large cell carcinoma. By learning transferable structure across tasks while preserving sample specific adaptability, our approach enables rapid adaptation to individual samples, improving predictive accuracy across diverse tumor subtypes while uncovering context dependent patterns of gene influence that may inform personalized therapy.
AI-Assisted Decision-Making for Clinical Assessment of Auto-Segmented Contour Quality
May 01, 2025Purpose: This study presents a Deep Learning (DL)-based quality assessment (QA) approach for evaluating auto-generated contours (auto-contours) in radiotherapy, with emphasis on Online Adaptive Radiotherapy (OART). Leveraging Bayesian Ordinal Classification (BOC) and calibrated uncertainty thresholds, the method enables confident QA predictions without relying on ground truth contours or extensive manual labeling. Methods: We developed a BOC model to classify auto-contour quality and quantify prediction uncertainty. A calibration step was used to optimize uncertainty thresholds that meet clinical accuracy needs. The method was validated under three data scenarios: no manual labels, limited labels, and extensive labels. For rectum contours in prostate cancer, we applied geometric surrogate labels when manual labels were absent, transfer learning when limited, and direct supervision when ample labels were available. Results: The BOC model delivered robust performance across all scenarios. Fine-tuning with just 30 manual labels and calibrating with 34 subjects yielded over 90% accuracy on test data. Using the calibrated threshold, over 93% of the auto-contours' qualities were accurately predicted in over 98% of cases, reducing unnecessary manual reviews and highlighting cases needing correction. Conclusion: The proposed QA model enhances contouring efficiency in OART by reducing manual workload and enabling fast, informed clinical decisions. Through uncertainty quantification, it ensures safer, more reliable radiotherapy workflows.
Understanding the PULSAR Effect in Combined Radiotherapy and Immunotherapy through Attention Mechanisms with a Transformer Model
Mar 07, 2024PULSAR (personalized, ultra-fractionated stereotactic adaptive radiotherapy) is the adaptation of stereotactic ablative radiotherapy towards personalized cancer management. For the first time, we applied a transformer-based attention mechanism to investigate the underlying interactions between combined PULSAR and PD-L1 blockade immunotherapy based on a murine cancer model (Lewis Lung Carcinoma, LLC). The proposed approach is able to predict the trend of tumor volume change semi-quantitatively, and excels in identifying the potential causal relationships through both self-attention and cross-attention scores.
Can input reconstruction be used to directly estimate uncertainty of a regression U-Net model? -- Application to proton therapy dose prediction for head and neck cancer patients
Oct 30, 2023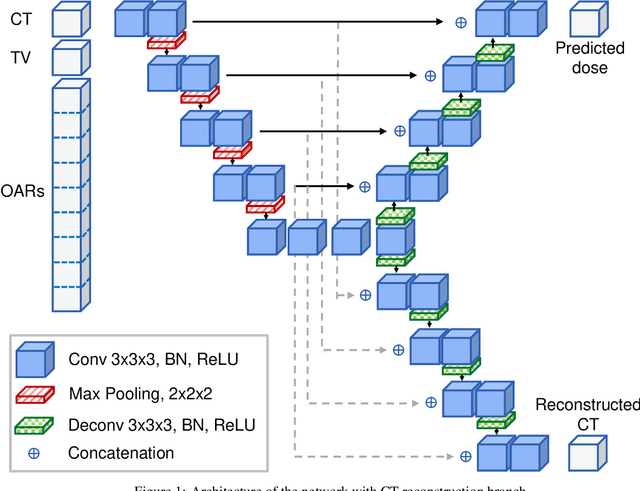


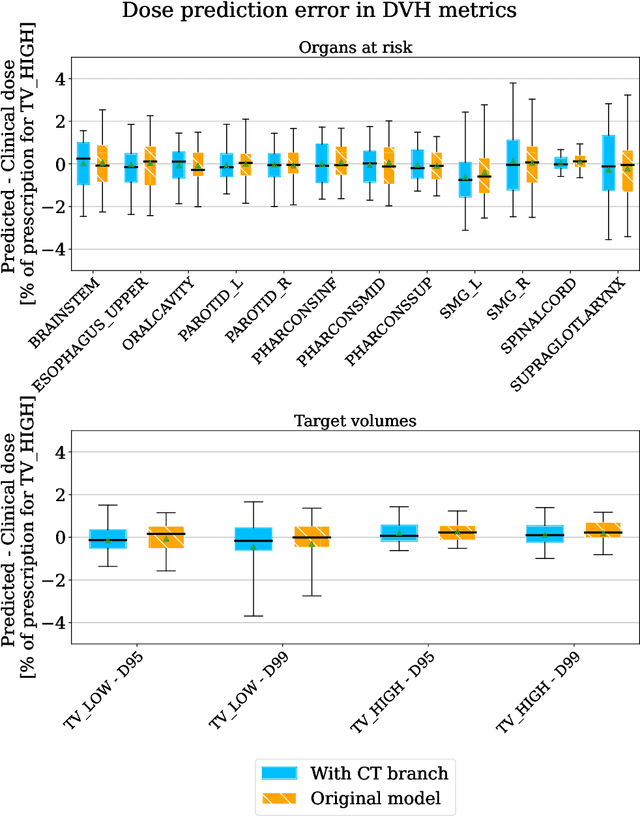
Estimating the uncertainty of deep learning models in a reliable and efficient way has remained an open problem, where many different solutions have been proposed in the literature. Most common methods are based on Bayesian approximations, like Monte Carlo dropout (MCDO) or Deep ensembling (DE), but they have a high inference time (i.e. require multiple inference passes) and might not work for out-of-distribution detection (OOD) data (i.e. similar uncertainty for in-distribution (ID) and OOD). In safety critical environments, like medical applications, accurate and fast uncertainty estimation methods, able to detect OOD data, are crucial, since wrong predictions can jeopardize patients safety. In this study, we present an alternative direct uncertainty estimation method and apply it for a regression U-Net architecture. The method consists in the addition of a branch from the bottleneck which reconstructs the input. The input reconstruction error can be used as a surrogate of the model uncertainty. For the proof-of-concept, our method is applied to proton therapy dose prediction in head and neck cancer patients. Accuracy, time-gain, and OOD detection are analyzed for our method in this particular application and compared with the popular MCDO and DE. The input reconstruction method showed a higher Pearson correlation coefficient with the prediction error (0.620) than DE and MCDO (between 0.447 and 0.612). Moreover, our method allows an easier identification of OOD (Z-score of 34.05). It estimates the uncertainty simultaneously to the regression task, therefore requires less time or computational resources.
Zero-shot Medical Image Translation via Frequency-Guided Diffusion Models
Apr 05, 2023



Recently, the diffusion model has emerged as a superior generative model that can produce high-quality images with excellent realism. There is a growing interest in applying diffusion models to image translation tasks. However, for medical image translation, the existing diffusion models are deficient in accurately retaining structural information since the structure details of source domain images are lost during the forward diffusion process and cannot be fully recovered through learned reverse diffusion, while the integrity of anatomical structures is extremely important in medical images. Training and conditioning diffusion models using paired source and target images with matching anatomy can help. However, such paired data are very difficult and costly to obtain, and may also reduce the robustness of the developed model to out-of-distribution testing data. We propose a frequency-guided diffusion model (FGDM) that employs frequency-domain filters to guide the diffusion model for structure-preserving image translation. Based on its design, FGDM allows zero-shot learning, as it can be trained solely on the data from the target domain, and used directly for source-to-target domain translation without any exposure to the source-domain data during training. We trained FGDM solely on the head-and-neck CT data, and evaluated it on both head-and-neck and lung cone-beam CT (CBCT)-to-CT translation tasks. FGDM outperformed the state-of-the-art methods (GAN-based, VAE-based, and diffusion-based) in all metrics, showing its significant advantages in zero-shot medical image translation.
Deep Learning (DL)-based Automatic Segmentation of the Internal Pudendal Artery (IPA) for Reduction of Erectile Dysfunction in Definitive Radiotherapy of Localized Prostate Cancer
Feb 03, 2023Background and purpose: Radiation-induced erectile dysfunction (RiED) is commonly seen in prostate cancer patients. Clinical trials have been developed in multiple institutions to investigate whether dose-sparing to the internal-pudendal-arteries (IPA) will improve retention of sexual potency. The IPA is usually not considered a conventional organ-at-risk (OAR) due to segmentation difficulty. In this work, we propose a deep learning (DL)-based auto-segmentation model for the IPA that utilizes CT and MRI or CT alone as the input image modality to accommodate variation in clinical practice. Materials and methods: 86 patients with CT and MRI images and noisy IPA labels were recruited in this study. We split the data into 42/14/30 for model training, testing, and a clinical observer study, respectively. There were three major innovations in this model: 1) we designed an architecture with squeeze-and-excite blocks and modality attention for effective feature extraction and production of accurate segmentation, 2) a novel loss function was used for training the model effectively with noisy labels, and 3) modality dropout strategy was used for making the model capable of segmentation in the absence of MRI. Results: The DSC, ASD, and HD95 values for the test dataset were 62.2%, 2.54mm, and 7mm, respectively. AI segmented contours were dosimetrically equivalent to the expert physician's contours. The observer study showed that expert physicians' scored AI contours (mean=3.7) higher than inexperienced physicians' contours (mean=3.1). When inexperienced physicians started with AI contours, the score improved to 3.7. Conclusion: The proposed model achieved good quality IPA contours to improve uniformity of segmentation and to facilitate introduction of standardized IPA segmentation into clinical trials and practice.
Prior Guided Deep Difference Meta-Learner for Fast Adaptation to Stylized Segmentation
Nov 19, 2022When a pre-trained general auto-segmentation model is deployed at a new institution, a support framework in the proposed Prior-guided DDL network will learn the systematic difference between the model predictions and the final contours revised and approved by clinicians for an initial group of patients. The learned style feature differences are concatenated with the new patients (query) features and then decoded to get the style-adapted segmentations. The model is independent of practice styles and anatomical structures. It meta-learns with simulated style differences and does not need to be exposed to any real clinical stylized structures during training. Once trained on the simulated data, it can be deployed for clinical use to adapt to new practice styles and new anatomical structures without further training. To show the proof of concept, we tested the Prior-guided DDL network on six different practice style variations for three different anatomical structures. Pre-trained segmentation models were adapted from post-operative clinical target volume (CTV) segmentation to segment CTVstyle1, CTVstyle2, and CTVstyle3, from parotid gland segmentation to segment Parotidsuperficial, and from rectum segmentation to segment Rectumsuperior and Rectumposterior. The mode performance was quantified with Dice Similarity Coefficient (DSC). With adaptation based on only the first three patients, the average DSCs were improved from 78.6, 71.9, 63.0, 52.2, 46.3 and 69.6 to 84.4, 77.8, 73.0, 77.8, 70.5, 68.1, for CTVstyle1, CTVstyle2, and CTVstyle3, Parotidsuperficial, Rectumsuperior, and Rectumposterior, respectively, showing the great potential of the Priorguided DDL network for a fast and effortless adaptation to new practice styles
Performance Deterioration of Deep Learning Models after Clinical Deployment: A Case Study with Auto-segmentation for Definitive Prostate Cancer Radiotherapy
Oct 11, 2022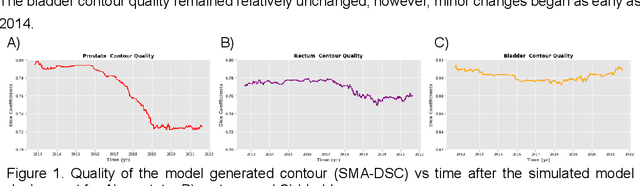
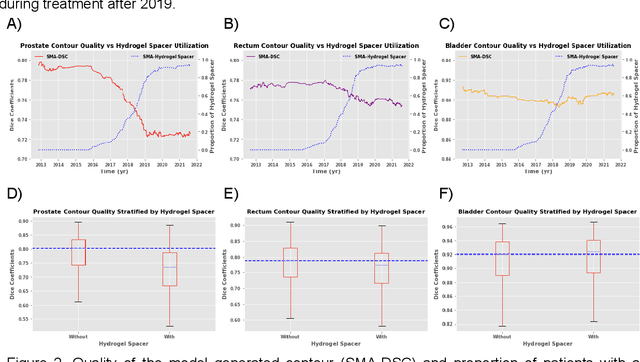
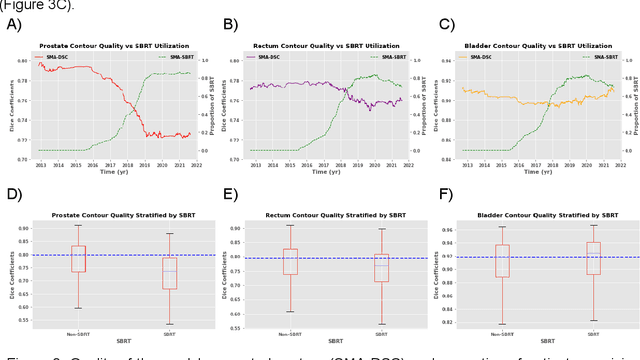
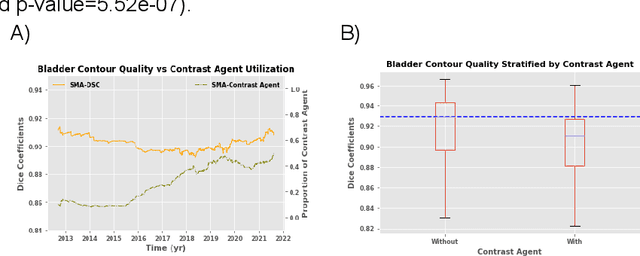
In the past decade, deep learning (DL)-based artificial intelligence (AI) has witnessed unprecedented success and has led to much excitement in medicine. However, many successful models have not been implemented in the clinic predominantly due to concerns regarding the lack of interpretability and generalizability in both spatial and temporal domains. In this work, we used a DL-based auto segmentation model for intact prostate patients to observe any temporal performance changes and then correlate them to possible explanatory variables. We retrospectively simulated the clinical implementation of our DL model to investigate temporal performance trends. Our cohort included 912 patients with prostate cancer treated with definitive radiotherapy from January 2006 to August 2021 at the University of Texas Southwestern Medical Center (UTSW). We trained a U-Net-based DL auto segmentation model on the data collected before 2012 and tested it on data collected from 2012 to 2021 to simulate the clinical deployment of the trained model starting in 2012. We visualize the trends using a simple moving average curve and used ANOVA and t-test to investigate the impact of various clinical factors. The prostate and rectum contour quality decreased rapidly after 2016-2017. Stereotactic body radiotherapy (SBRT) and hydrogel spacer use were significantly associated with prostate contour quality (p=5.6e-12 and 0.002, respectively). SBRT and physicians' styles are significantly associated with the rectum contour quality (p=0.0005 and 0.02, respectively). Only the presence of contrast within the bladder significantly affected the bladder contour quality (p=1.6e-7). We showed that DL model performance decreased over time in concordance with changes in clinical practice patterns and changes in clinical personnel.
Uncertainty estimations methods for a deep learning model to aid in clinical decision-making -- a clinician's perspective
Oct 02, 2022



Prediction uncertainty estimation has clinical significance as it can potentially quantify prediction reliability. Clinicians may trust 'blackbox' models more if robust reliability information is available, which may lead to more models being adopted into clinical practice. There are several deep learning-inspired uncertainty estimation techniques, but few are implemented on medical datasets -- fewer on single institutional datasets/models. We sought to compare dropout variational inference (DO), test-time augmentation (TTA), conformal predictions, and single deterministic methods for estimating uncertainty using our model trained to predict feeding tube placement for 271 head and neck cancer patients treated with radiation. We compared the area under the curve (AUC), sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) trends for each method at various cutoffs that sought to stratify patients into 'certain' and 'uncertain' cohorts. These cutoffs were obtained by calculating the percentile "uncertainty" within the validation cohort and applied to the testing cohort. Broadly, the AUC, sensitivity, and NPV increased as the predictions were more 'certain' -- i.e., lower uncertainty estimates. However, when a majority vote (implementing 2/3 criteria: DO, TTA, conformal predictions) or a stricter approach (3/3 criteria) were used, AUC, sensitivity, and NPV improved without a notable loss in specificity or PPV. Especially for smaller, single institutional datasets, it may be important to evaluate multiple estimations techniques before incorporating a model into clinical practice.