 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeAttentive Q-Matrix Learning for Knowledge Tracing
Apr 06, 2023As the rapid development of Intelligent Tutoring Systems (ITS) in the past decade, tracing the students' knowledge state has become more and more important in order to provide individualized learning guidance. This is the main idea of Knowledge Tracing (KT), which models students' mastery of knowledge concepts (KCs, skills needed to solve a question) based on their past interactions on platforms. Plenty of KT models have been proposed and have shown remarkable performance recently. However, the majority of these models use concepts to index questions, which means the predefined skill tags for each question are required in advance to indicate the KCs needed to answer that question correctly. This makes it pretty hard to apply on large-scale online education platforms where questions are often not well-organized by skill tags. In this paper, we propose Q-matrix-based Attentive Knowledge Tracing (QAKT), an end-to-end style model that is able to apply the attentive method to scenes where no predefined skill tags are available without sacrificing its performance. With a novel hybrid embedding method based on the q-matrix and Rasch model, QAKT is capable of modeling problems hierarchically and learning the q-matrix efficiently based on students' sequences. Meanwhile, the architecture of QAKT ensures that it is friendly to questions associated with multiple skills and has outstanding interpretability. After conducting experiments on a variety of open datasets, we empirically validated that our model shows similar or even better performance than state-of-the-art KT methods. Results of further experiments suggest that the q-matrix learned by QAKT is highly model-agnostic and more information-sufficient than the one labeled by human experts, which could help with the data mining tasks in existing ITSs.
ULDor: A Universal Lesion Detector for CT Scans with Pseudo Masks and Hard Negative Example Mining
Jan 18, 2019


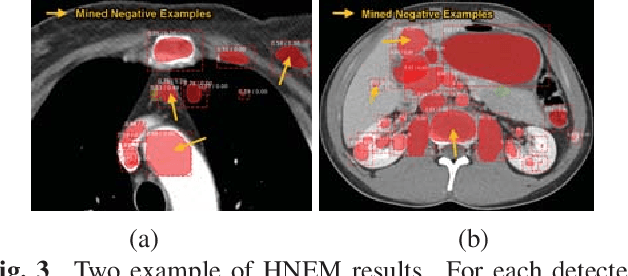
Automatic lesion detection from computed tomography (CT) scans is an important task in medical imaging analysis. It is still very challenging due to similar appearances (e.g. intensity and texture) between lesions and other tissues, making it especially difficult to develop a universal lesion detector. Instead of developing a specific-type lesion detector, this work builds a Universal Lesion Detector (ULDor) based on Mask R-CNN, which is able to detect all different kinds of lesions from whole body parts. As a state-of-the-art object detector, Mask R-CNN adds a branch for predicting segmentation masks on each Region of Interest (RoI) to improve the detection performance. However, it is almost impossible to manually annotate a large-scale dataset with pixel-level lesion masks to train the Mask R-CNN for lesion detection. To address this problem, this work constructs a pseudo mask for each lesion region that can be considered as a surrogate of the real mask, based on which the Mask R-CNN is employed for lesion detection. On the other hand, this work proposes a hard negative example mining strategy to reduce the false positives for improving the detection performance. Experimental results on the NIH DeepLesion dataset demonstrate that the ULDor is enhanced using pseudo masks and the proposed hard negative example mining strategy and achieves a sensitivity of 86.21% with five false positives per image.
A Bottom-up Approach for Pancreas Segmentation using Cascaded Superpixels and (Deep) Image Patch Labeling
Mar 07, 2016

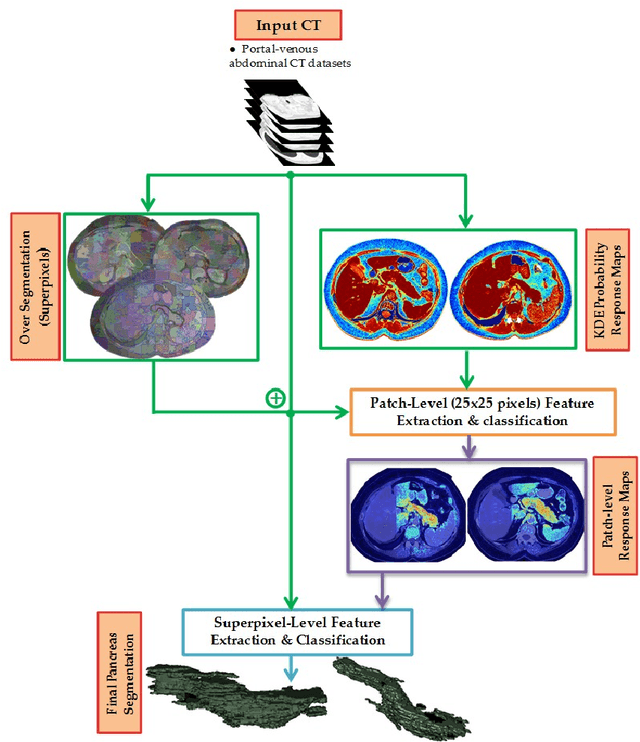
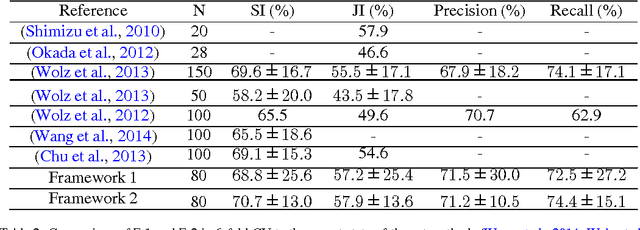
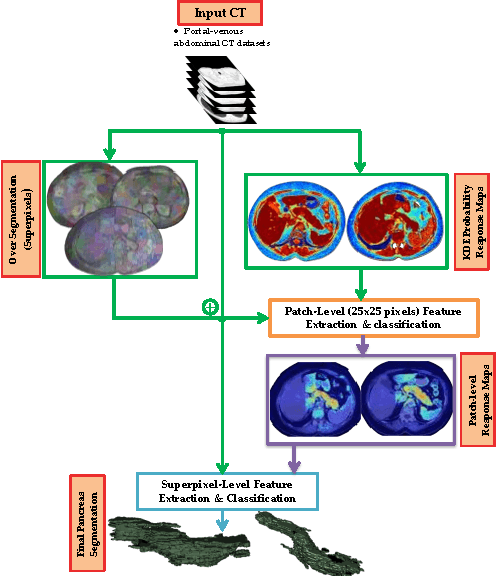
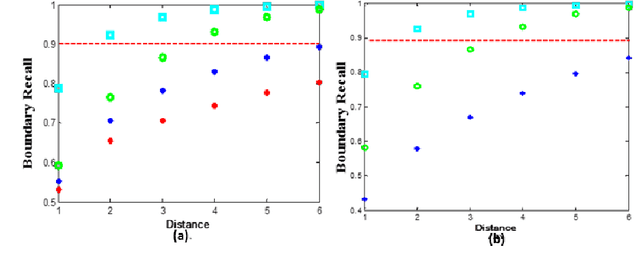
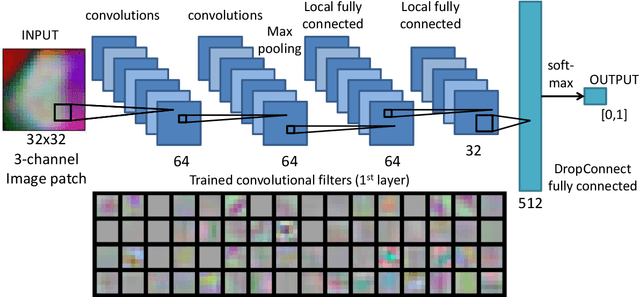
Robust automated organ segmentation is a prerequisite for computer-aided diagnosis (CAD), quantitative imaging analysis and surgical assistance. For high-variability organs such as the pancreas, previous approaches report undesirably low accuracies. We present a bottom-up approach for pancreas segmentation in abdominal CT scans that is based on a hierarchy of information propagation by classifying image patches at different resolutions; and cascading superpixels. There are four stages: 1) decomposing CT slice images as a set of disjoint boundary-preserving superpixels; 2) computing pancreas class probability maps via dense patch labeling; 3) classifying superpixels by pooling both intensity and probability features to form empirical statistics in cascaded random forest frameworks; and 4) simple connectivity based post-processing. The dense image patch labeling are conducted by: efficient random forest classifier on image histogram, location and texture features; and more expensive (but with better specificity) deep convolutional neural network classification on larger image windows (with more spatial contexts). Evaluation of the approach is performed on a database of 80 manually segmented CT volumes in six-fold cross-validation (CV). Our achieved results are comparable, or better than the state-of-the-art methods (evaluated by "leave-one-patient-out"), with Dice 70.7% and Jaccard 57.9%. The computational efficiency has been drastically improved in the order of 6~8 minutes, comparing with others of ~10 hours per case. Finally, we implement a multi-atlas label fusion (MALF) approach for pancreas segmentation using the same datasets. Under six-fold CV, our bottom-up segmentation method significantly outperforms its MALF counterpart: (70.7 +/- 13.0%) versus (52.5 +/- 20.8%) in Dice. Deep CNN patch labeling confidences offer more numerical stability, reflected by smaller standard deviations.
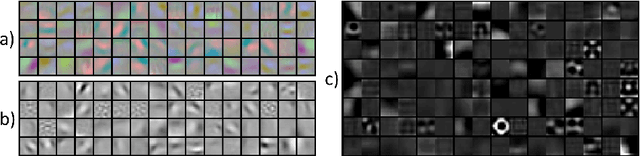
Improving Computer-aided Detection using Convolutional Neural Networks and Random View Aggregation
Sep 15, 2015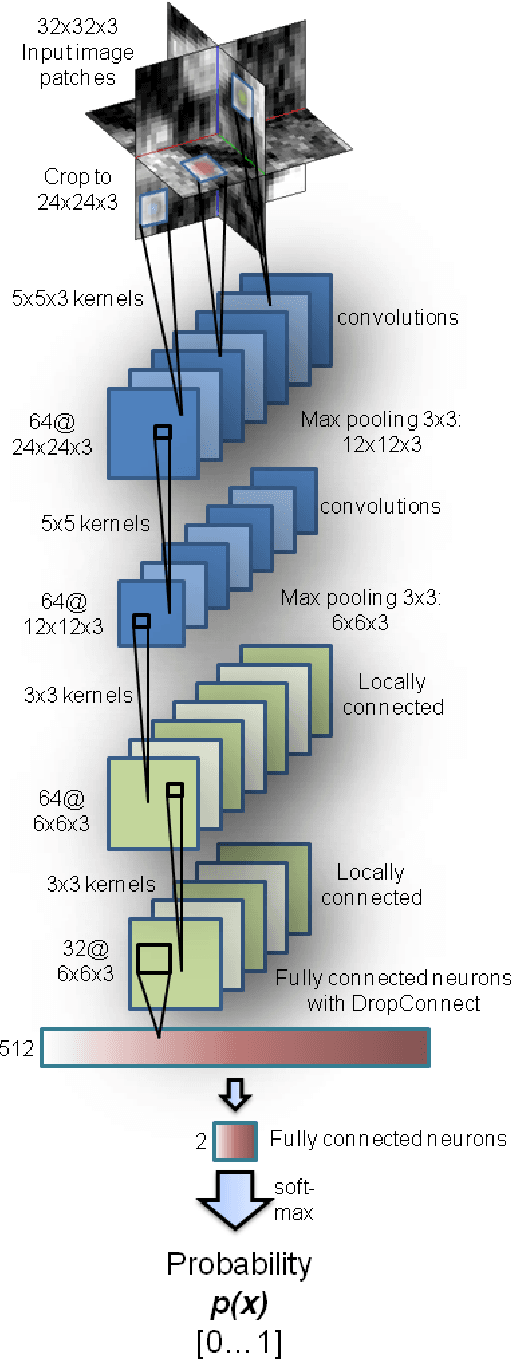


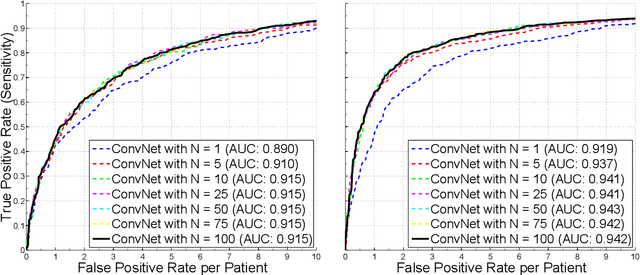
Automated computer-aided detection (CADe) in medical imaging has been an important tool in clinical practice and research. State-of-the-art methods often show high sensitivities but at the cost of high false-positives (FP) per patient rates. We design a two-tiered coarse-to-fine cascade framework that first operates a candidate generation system at sensitivities of $\sim$100% but at high FP levels. By leveraging existing CAD systems, coordinates of regions or volumes of interest (ROI or VOI) for lesion candidates are generated in this step and function as input for a second tier, which is our focus in this study. In this second stage, we generate $N$ 2D (two-dimensional) or 2.5D views via sampling through scale transformations, random translations and rotations with respect to each ROI's centroid coordinates. These random views are used to train deep convolutional neural network (ConvNet) classifiers. In testing, the trained ConvNets are employed to assign class (e.g., lesion, pathology) probabilities for a new set of $N$ random views that are then averaged at each ROI to compute a final per-candidate classification probability. This second tier behaves as a highly selective process to reject difficult false positives while preserving high sensitivities. The methods are evaluated on three different data sets with different numbers of patients: 59 patients for sclerotic metastases detection, 176 patients for lymph node detection, and 1,186 patients for colonic polyp detection. Experimental results show the ability of ConvNets to generalize well to different medical imaging CADe applications and scale elegantly to various data sets. Our proposed methods improve CADe performance markedly in all cases. CADe sensitivities improved from 57% to 70%, from 43% to 77% and from 58% to 75% at 3 FPs per patient for sclerotic metastases, lymph nodes and colonic polyps, respectively.
* 2D vs 2.5D vs 3D inputs and comparison to other standard classifiers such as SVM have been addressed by more experimentation and two completely new sections and figures. Results and Discussions have been updated accordingly
DeepOrgan: Multi-level Deep Convolutional Networks for Automated Pancreas Segmentation
Jun 22, 2015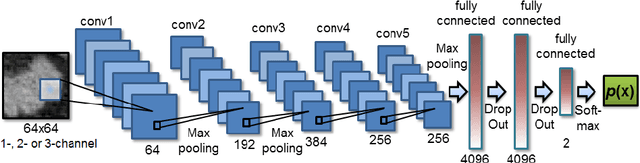
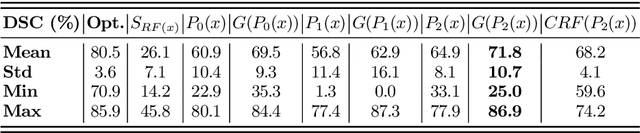

Automatic organ segmentation is an important yet challenging problem for medical image analysis. The pancreas is an abdominal organ with very high anatomical variability. This inhibits previous segmentation methods from achieving high accuracies, especially compared to other organs such as the liver, heart or kidneys. In this paper, we present a probabilistic bottom-up approach for pancreas segmentation in abdominal computed tomography (CT) scans, using multi-level deep convolutional networks (ConvNets). We propose and evaluate several variations of deep ConvNets in the context of hierarchical, coarse-to-fine classification on image patches and regions, i.e. superpixels. We first present a dense labeling of local image patches via $P{-}\mathrm{ConvNet}$ and nearest neighbor fusion. Then we describe a regional ConvNet ($R_1{-}\mathrm{ConvNet}$) that samples a set of bounding boxes around each image superpixel at different scales of contexts in a "zoom-out" fashion. Our ConvNets learn to assign class probabilities for each superpixel region of being pancreas. Last, we study a stacked $R_2{-}\mathrm{ConvNet}$ leveraging the joint space of CT intensities and the $P{-}\mathrm{ConvNet}$ dense probability maps. Both 3D Gaussian smoothing and 2D conditional random fields are exploited as structured predictions for post-processing. We evaluate on CT images of 82 patients in 4-fold cross-validation. We achieve a Dice Similarity Coefficient of 83.6$\pm$6.3% in training and 71.8$\pm$10.7% in testing.
2D View Aggregation for Lymph Node Detection Using a Shallow Hierarchy of Linear Classifiers
Aug 14, 2014

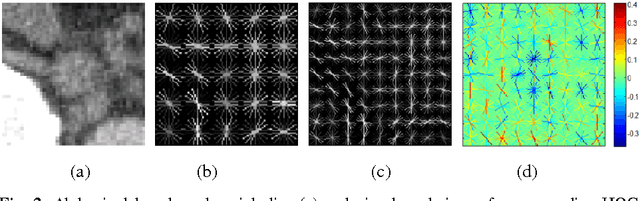
Enlarged lymph nodes (LNs) can provide important information for cancer diagnosis, staging, and measuring treatment reactions, making automated detection a highly sought goal. In this paper, we propose a new algorithm representation of decomposing the LN detection problem into a set of 2D object detection subtasks on sampled CT slices, largely alleviating the curse of dimensionality issue. Our 2D detection can be effectively formulated as linear classification on a single image feature type of Histogram of Oriented Gradients (HOG), covering a moderate field-of-view of 45 by 45 voxels. We exploit both simple pooling and sparse linear fusion schemes to aggregate these 2D detection scores for the final 3D LN detection. In this manner, detection is more tractable and does not need to perform perfectly at instance level (as weak hypotheses) since our aggregation process will robustly harness collective information for LN detection. Two datasets (90 patients with 389 mediastinal LNs and 86 patients with 595 abdominal LNs) are used for validation. Cross-validation demonstrates 78.0% sensitivity at 6 false positives/volume (FP/vol.) (86.1% at 10 FP/vol.) and 73.1% sensitivity at 6 FP/vol. (87.2% at 10 FP/vol.), for the mediastinal and abdominal datasets respectively. Our results compare favorably to previous state-of-the-art methods.
A Bottom-Up Approach for Automatic Pancreas Segmentation in Abdominal CT Scans
Jul 31, 2014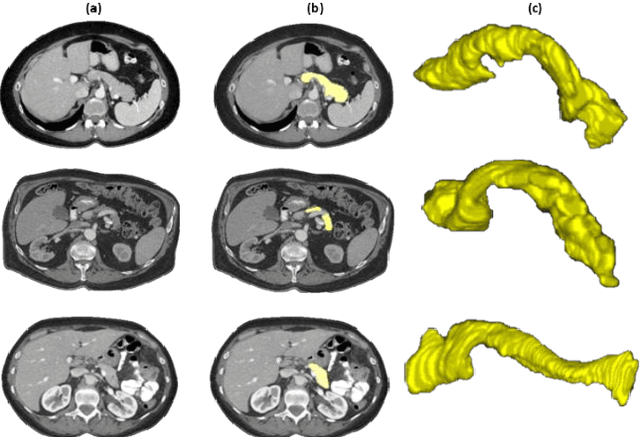
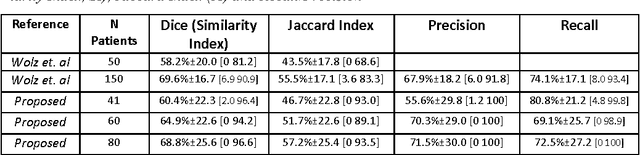
Organ segmentation is a prerequisite for a computer-aided diagnosis (CAD) system to detect pathologies and perform quantitative analysis. For anatomically high-variability abdominal organs such as the pancreas, previous segmentation works report low accuracies when comparing to organs like the heart or liver. In this paper, a fully-automated bottom-up method is presented for pancreas segmentation, using abdominal computed tomography (CT) scans. The method is based on a hierarchical two-tiered information propagation by classifying image patches. It labels superpixels as pancreas or not via pooling patch-level confidences on 2D CT slices over-segmented by the Simple Linear Iterative Clustering approach. A supervised random forest (RF) classifier is trained on the patch level and a two-level cascade of RFs is applied at the superpixel level, coupled with multi-channel feature extraction, respectively. On six-fold cross-validation using 80 patient CT volumes, we achieved 68.8% Dice coefficient and 57.2% Jaccard Index, comparable to or slightly better than published state-of-the-art methods.
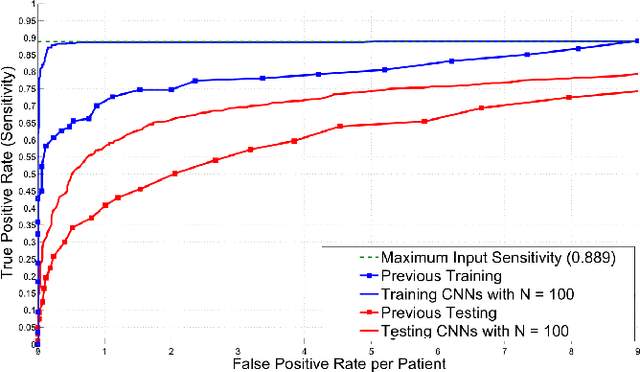
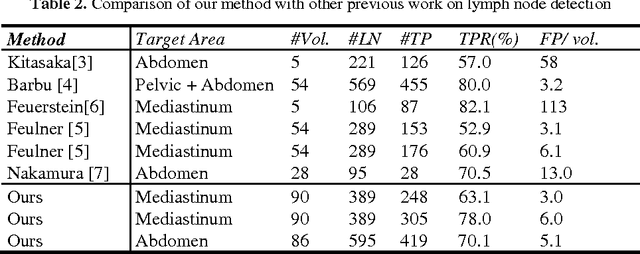
A New 2.5D Representation for Lymph Node Detection using Random Sets of Deep Convolutional Neural Network Observations
Jun 06, 2014

Automated Lymph Node (LN) detection is an important clinical diagnostic task but very challenging due to the low contrast of surrounding structures in Computed Tomography (CT) and to their varying sizes, poses, shapes and sparsely distributed locations. State-of-the-art studies show the performance range of 52.9% sensitivity at 3.1 false-positives per volume (FP/vol.), or 60.9% at 6.1 FP/vol. for mediastinal LN, by one-shot boosting on 3D HAAR features. In this paper, we first operate a preliminary candidate generation stage, towards 100% sensitivity at the cost of high FP levels (40 per patient), to harvest volumes of interest (VOI). Our 2.5D approach consequently decomposes any 3D VOI by resampling 2D reformatted orthogonal views N times, via scale, random translations, and rotations with respect to the VOI centroid coordinates. These random views are then used to train a deep Convolutional Neural Network (CNN) classifier. In testing, the CNN is employed to assign LN probabilities for all N random views that can be simply averaged (as a set) to compute the final classification probability per VOI. We validate the approach on two datasets: 90 CT volumes with 388 mediastinal LNs and 86 patients with 595 abdominal LNs. We achieve sensitivities of 70%/83% at 3 FP/vol. and 84%/90% at 6 FP/vol. in mediastinum and abdomen respectively, which drastically improves over the previous state-of-the-art work.
* This article will be presented at MICCAI (Medical Image Computing and Computer-Assisted Interventions) 2014