 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeOffline identification of surgical deviations in laparoscopic rectopexy
Sep 24, 2019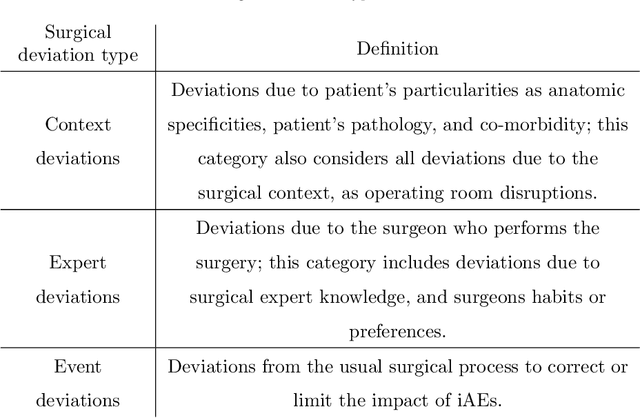
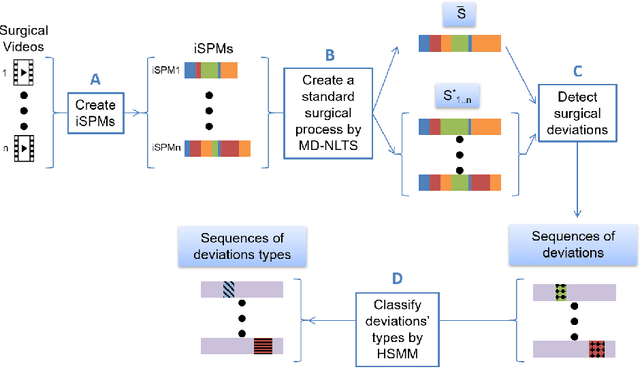
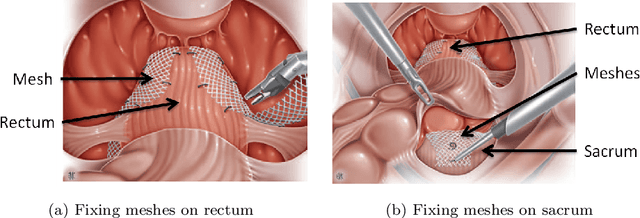
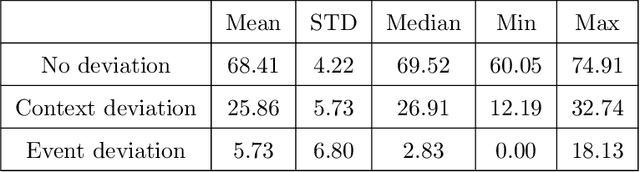
Objective: A median of 14.4% of patient undergone at least one adverse event during surgery and a third of them are preventable. The occurrence of adverse events forces surgeons to implement corrective strategies and, thus, deviate from the standard surgical process. Therefore, it is clear that the automatic identification of adverse events is a major challenge for patient safety. In this paper, we have proposed a method enabling us to identify such deviations. We have focused on identifying surgeons' deviations from standard surgical processes due to surgical events rather than anatomic specificities. This is particularly challenging, given the high variability in typical surgical procedure workflows. Methods: We have introduced a new approach designed to automatically detect and distinguish surgical process deviations based on multi-dimensional non-linear temporal scaling with a hidden semi-Markov model using manual annotation of surgical processes. The approach was then evaluated using cross-validation. Results: The best results have over 90% accuracy. Recall and precision were superior at 70%. We have provided a detailed analysis of the incorrectly-detected observations. Conclusion: Multi-dimensional non-linear temporal scaling with a hidden semi-Markov model provides promising results for detecting deviations. Our error analysis of the incorrectly-detected observations offers different leads in order to further improve our method. Significance: Our method demonstrated the feasibility of automatically detecting surgical deviations that could be implemented for both skill analysis and developing situation awareness-based computer-assisted surgical systems.
Comparative evaluation of instrument segmentation and tracking methods in minimally invasive surgery
May 07, 2018
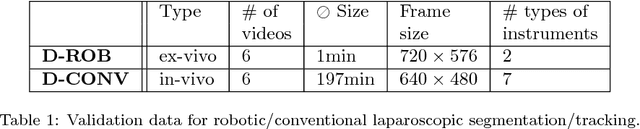

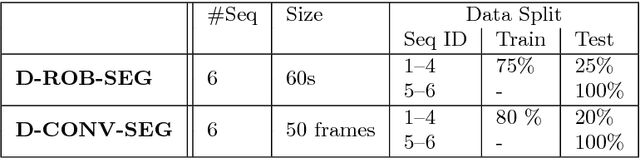
Intraoperative segmentation and tracking of minimally invasive instruments is a prerequisite for computer- and robotic-assisted surgery. Since additional hardware like tracking systems or the robot encoders are cumbersome and lack accuracy, surgical vision is evolving as promising techniques to segment and track the instruments using only the endoscopic images. However, what is missing so far are common image data sets for consistent evaluation and benchmarking of algorithms against each other. The paper presents a comparative validation study of different vision-based methods for instrument segmentation and tracking in the context of robotic as well as conventional laparoscopic surgery. The contribution of the paper is twofold: we introduce a comprehensive validation data set that was provided to the study participants and present the results of the comparative validation study. Based on the results of the validation study, we arrive at the conclusion that modern deep learning approaches outperform other methods in instrument segmentation tasks, but the results are still not perfect. Furthermore, we show that merging results from different methods actually significantly increases accuracy in comparison to the best stand-alone method. On the other hand, the results of the instrument tracking task show that this is still an open challenge, especially during challenging scenarios in conventional laparoscopic surgery.
First Clinical Experience in Urologic Surgery with a Novel Robotic Lightweight Laparoscope Holder
Aug 31, 2012
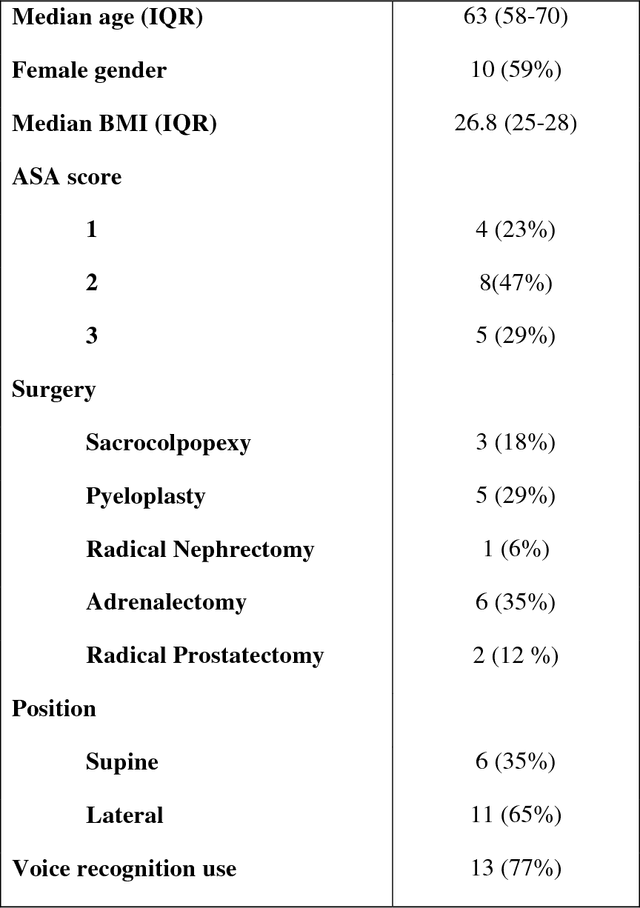


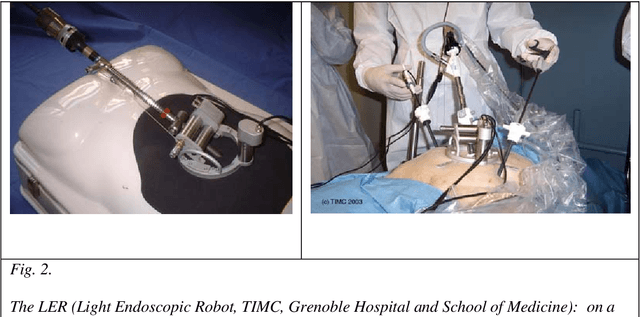
Purpose: To report the feasibility and the safety of a surgeon-controlled robotic endoscope holder in laparoscopic surgery. Materials and methods: From March 2010 to September 2010, 20 patients were enrolled prospectively to undergo a laparoscopic surgery using an innovative robotic endoscope holder. Two surgeons performed 6 adrenalectomies, 4 sacrocolpopexies, 5 pyeloplasties, 4 radical prostatectomies and 1 radical nephrectomy. Demographic data, overall set-up time, operative time, number of assistants needed were reviewed. Surgeon's satisfaction regarding the ergonomics was assessed using a ten point scale. Postoperative clinical outcomes were reviewed at day 1 and 1 month postoperatively. Results: The per-protocol analysis was performed on 17 patients for whom the robot was effectively used for surgery. Median age was 63 years, 10 patients were female (59%). Median BMI was 26.8. Surgical procedures were completed with the robot in 12 cases (71 %). Median number of surgical assistant was 0. Overall set-up time with the robot was 19 min, operative time was 130 min) during which the robot was used 71% of the time. Mean hospital stay was 6.94 days $\pm$ 2.3. Median score regarding the easiness of use was 7. Median pain level was 1.5/10 at day 1 and 0 at 1 month postoperatively. Open conversion was needed in 1 case (6 %) and 4 minor complications occurred in 2 patients (12%). Conclusion: This use of this novel robotic laparoscope holder is safe, feasible and it provides a good comfort to the surgeon.
Medical image computing and computer-aided medical interventions applied to soft tissues. Work in progress in urology
Dec 13, 2007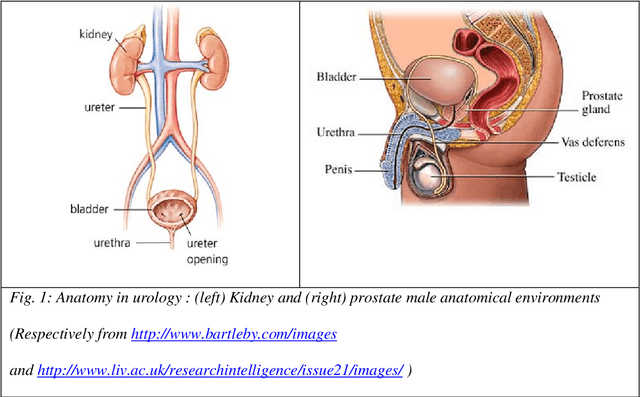
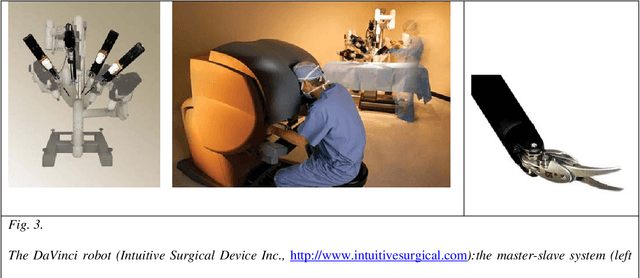

Until recently, Computer-Aided Medical Interventions (CAMI) and Medical Robotics have focused on rigid and non deformable anatomical structures. Nowadays, special attention is paid to soft tissues, raising complex issues due to their mobility and deformation. Mini-invasive digestive surgery was probably one of the first fields where soft tissues were handled through the development of simulators, tracking of anatomical structures and specific assistance robots. However, other clinical domains, for instance urology, are concerned. Indeed, laparoscopic surgery, new tumour destruction techniques (e.g. HIFU, radiofrequency, or cryoablation), increasingly early detection of cancer, and use of interventional and diagnostic imaging modalities, recently opened new challenges to the urologist and scientists involved in CAMI. This resulted in the last five years in a very significant increase of research and developments of computer-aided urology systems. In this paper, we propose a description of the main problems related to computer-aided diagnostic and therapy of soft tissues and give a survey of the different types of assistance offered to the urologist: robotization, image fusion, surgical navigation. Both research projects and operational industrial systems are discussed.