 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeInjecting knowledge into language generation: a case study in auto-charting after-visit care instructions from medical dialogue
Jun 06, 2023



Factual correctness is often the limiting factor in practical applications of natural language generation in high-stakes domains such as healthcare. An essential requirement for maintaining factuality is the ability to deal with rare tokens. This paper focuses on rare tokens that appear in both the source and the reference sequences, and which, when missed during generation, decrease the factual correctness of the output text. For high-stake domains that are also knowledge-rich, we show how to use knowledge to (a) identify which rare tokens that appear in both source and reference are important and (b) uplift their conditional probability. We introduce the ``utilization rate'' that encodes knowledge and serves as a regularizer by maximizing the marginal probability of selected tokens. We present a study in a knowledge-rich domain of healthcare, where we tackle the problem of generating after-visit care instructions based on patient-doctor dialogues. We verify that, in our dataset, specific medical concepts with high utilization rates are underestimated by conventionally trained sequence-to-sequence models. We observe that correcting this with our approach to knowledge injection reduces the uncertainty of the model as well as improves factuality and coherence without negatively impacting fluency.
Dialogue-Contextualized Re-ranking for Medical History-Taking
Apr 04, 2023



AI-driven medical history-taking is an important component in symptom checking, automated patient intake, triage, and other AI virtual care applications. As history-taking is extremely varied, machine learning models require a significant amount of data to train. To overcome this challenge, existing systems are developed using indirect data or expert knowledge. This leads to a training-inference gap as models are trained on different kinds of data than what they observe at inference time. In this work, we present a two-stage re-ranking approach that helps close the training-inference gap by re-ranking the first-stage question candidates using a dialogue-contextualized model. For this, we propose a new model, global re-ranker, which cross-encodes the dialogue with all questions simultaneously, and compare it with several existing neural baselines. We test both transformer and S4-based language model backbones. We find that relative to the expert system, the best performance is achieved by our proposed global re-ranker with a transformer backbone, resulting in a 30% higher normalized discount cumulative gain (nDCG) and a 77% higher mean average precision (mAP).
Learning functional sections in medical conversations: iterative pseudo-labeling and human-in-the-loop approach
Oct 07, 2022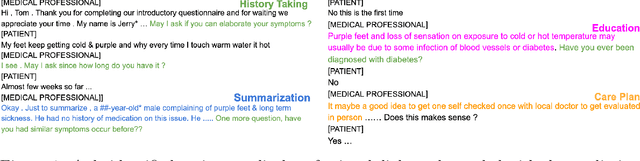
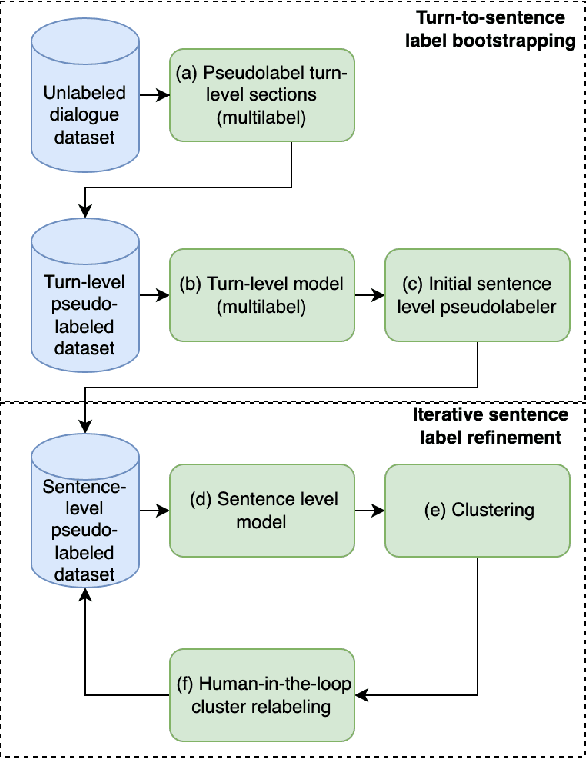
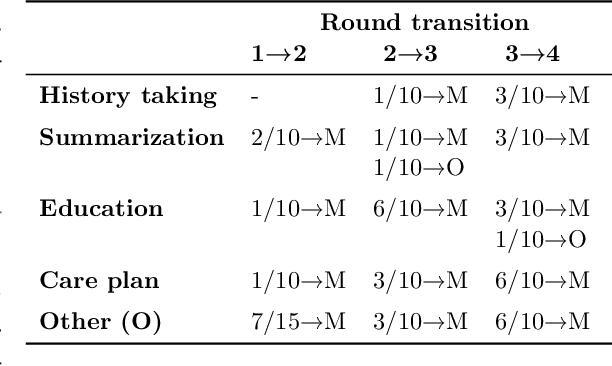
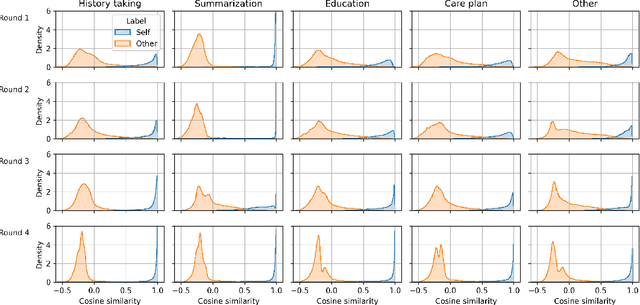
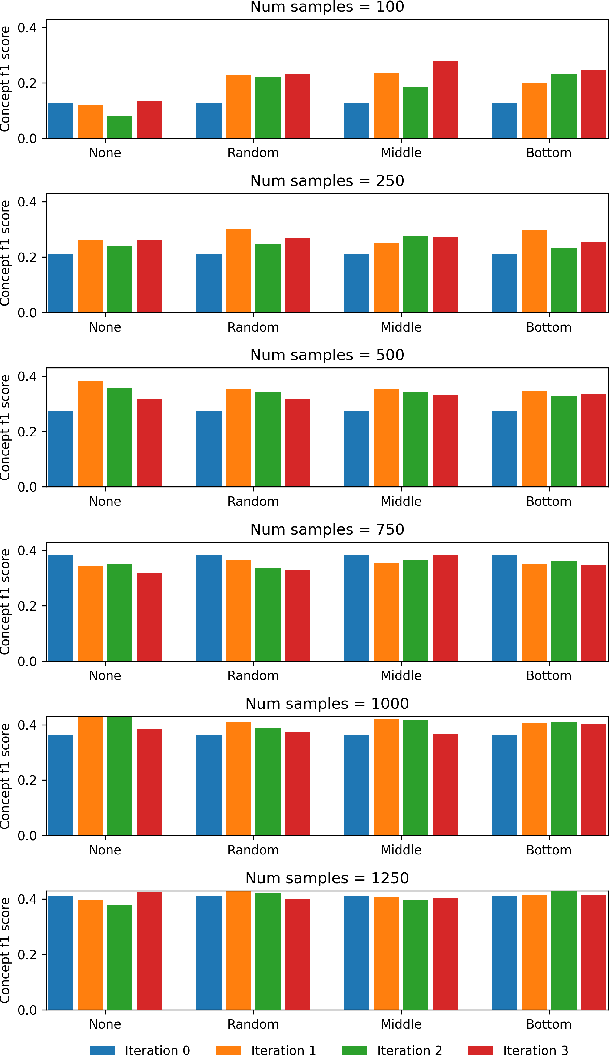
Medical conversations between patients and medical professionals have implicit functional sections, such as "history taking", "summarization", "education", and "care plan." In this work, we are interested in learning to automatically extract these sections. A direct approach would require collecting large amounts of expert annotations for this task, which is inherently costly due to the contextual inter-and-intra variability between these sections. This paper presents an approach that tackles the problem of learning to classify medical dialogue into functional sections without requiring a large number of annotations. Our approach combines pseudo-labeling and human-in-the-loop. First, we bootstrap using weak supervision with pseudo-labeling to generate dialogue turn-level pseudo-labels and train a transformer-based model, which is then applied to individual sentences to create noisy sentence-level labels. Second, we iteratively refine sentence-level labels using a cluster-based human-in-the-loop approach. Each iteration requires only a few dozen annotator decisions. We evaluate the results on an expert-annotated dataset of 100 dialogues and find that while our models start with 69.5% accuracy, we can iteratively improve it to 82.5%. The code used to perform all experiments described in this paper can be found here: https://github.com/curai/curai-research/tree/main/functional-sections.
OSLAT: Open Set Label Attention Transformer for Medical Entity Span Extraction
Jul 12, 2022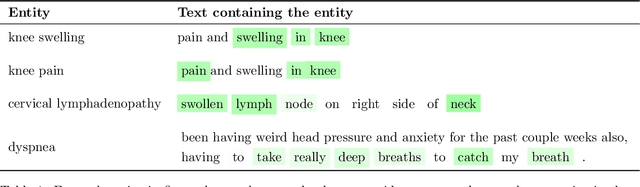
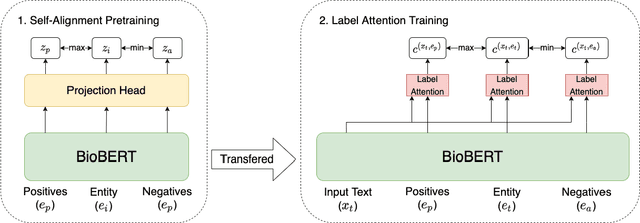
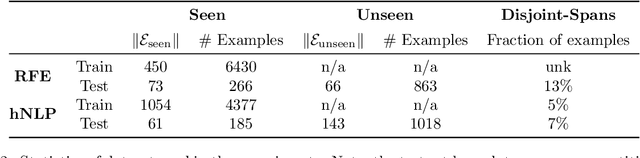
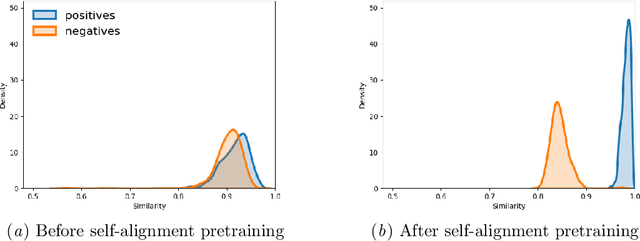
Identifying spans in medical texts that correspond to medical entities is one of the core steps for many healthcare NLP tasks such as ICD coding, medical finding extraction, medical note contextualization, to name a few. Existing entity extraction methods rely on a fixed and limited vocabulary of medical entities and have difficulty with extracting entities represented by disjoint spans. In this paper, we present a new transformer-based architecture called OSLAT, Open Set Label Attention Transformer, that addresses many of the limitations of the previous methods. Our approach uses the label-attention mechanism to implicitly learn spans associated with entities of interest. These entities can be provided as free text, including entities not seen during OSLAT's training, and the model can extract spans even when they are disjoint. To test the generalizability of our method, we train two separate models on two different datasets, which have very low entity overlap: (1) a public discharge notes dataset from hNLP, and (2) a much more challenging proprietary patient text dataset "Reasons for Encounter" (RFE). We find that OSLAT models trained on either dataset outperform rule-based and fuzzy string matching baselines when applied to the RFE dataset as well as to the portion of hNLP dataset where entities are represented by disjoint spans. Our code can be found at https://github.com/curai/curai-research/tree/main/OSLAT.
Adding more data does not always help: A study in medical conversation summarization with PEGASUS
Nov 28, 2021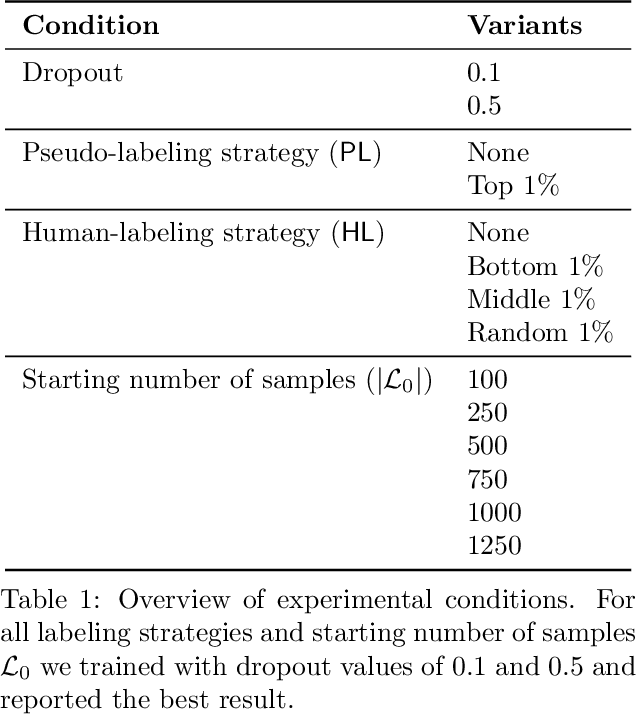

Medical conversation summarization is integral in capturing information gathered during interactions between patients and physicians. Summarized conversations are used to facilitate patient hand-offs between physicians, and as part of providing care in the future. Summaries, however, can be time-consuming to produce and require domain expertise. Modern pre-trained NLP models such as PEGASUS have emerged as capable alternatives to human summarization, reaching state-of-the-art performance on many summarization benchmarks. However, many downstream tasks still require at least moderately sized datasets to achieve satisfactory performance. In this work we (1) explore the effect of dataset size on transfer learning medical conversation summarization using PEGASUS and (2) evaluate various iterative labeling strategies in the low-data regime, following their success in the classification setting. We find that model performance saturates with increase in dataset size and that the various active-learning strategies evaluated all show equivalent performance consistent with simple dataset size increase. We also find that naive iterative pseudo-labeling is on-par or slightly worse than no pseudo-labeling. Our work sheds light on the successes and challenges of translating low-data regime techniques in classification to medical conversation summarization and helps guides future work in this space. Relevant code available at \url{https://github.com/curai/curai-research/tree/main/medical-summarization-ML4H-2021}.
MEDCOD: A Medically-Accurate, Emotive, Diverse, and Controllable Dialog System
Nov 17, 2021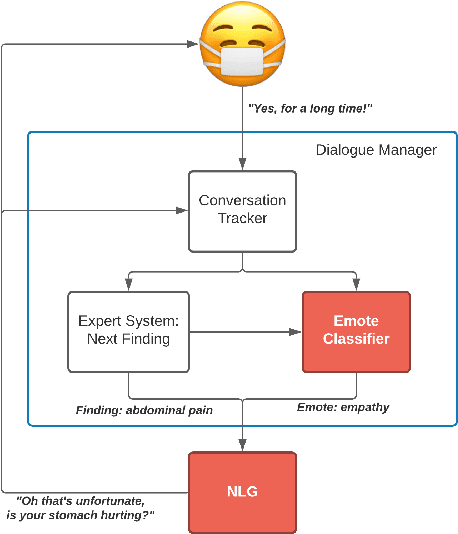


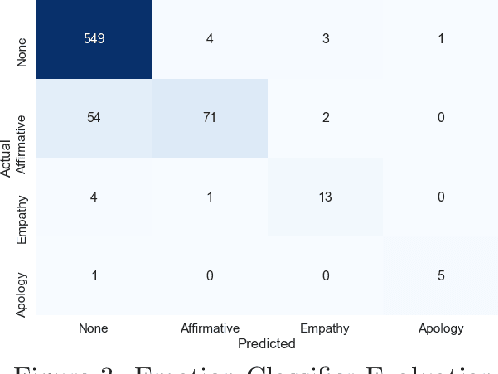
We present MEDCOD, a Medically-Accurate, Emotive, Diverse, and Controllable Dialog system with a unique approach to the natural language generator module. MEDCOD has been developed and evaluated specifically for the history taking task. It integrates the advantage of a traditional modular approach to incorporate (medical) domain knowledge with modern deep learning techniques to generate flexible, human-like natural language expressions. Two key aspects of MEDCOD's natural language output are described in detail. First, the generated sentences are emotive and empathetic, similar to how a doctor would communicate to the patient. Second, the generated sentence structures and phrasings are varied and diverse while maintaining medical consistency with the desired medical concept (provided by the dialogue manager module of MEDCOD). Experimental results demonstrate the effectiveness of our approach in creating a human-like medical dialogue system. Relevant code is available at https://github.com/curai/curai-research/tree/main/MEDCOD
SmartTriage: A system for personalized patient data capture, documentation generation, and decision support
Oct 19, 2020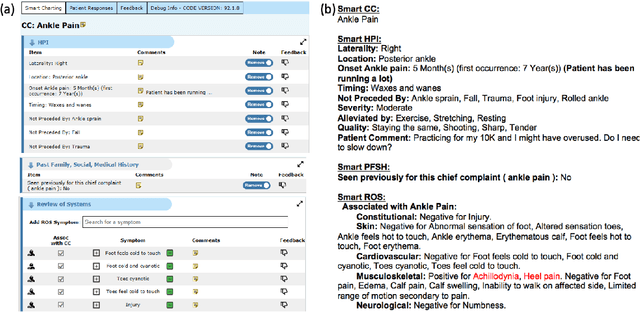
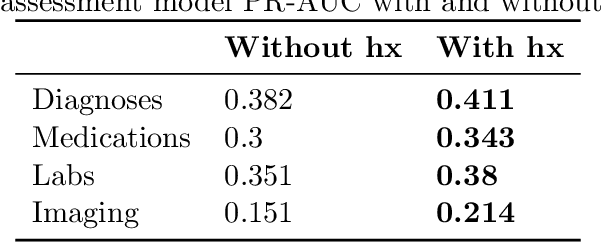
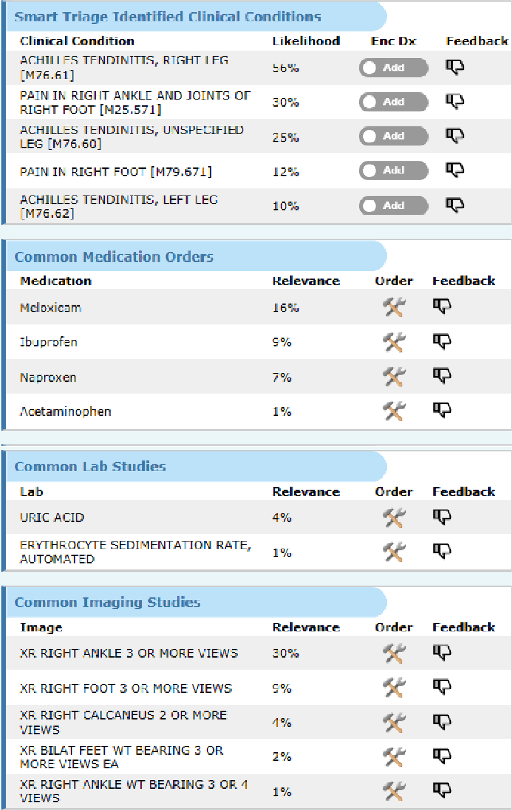
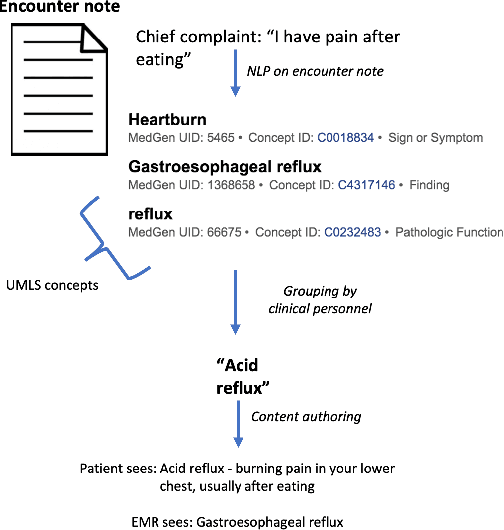
Symptom checkers have emerged as an important tool for collecting symptoms and diagnosing patients, minimizing the involvement of clinical personnel. We developed a machine-learning-backed system, SmartTriage, which goes beyond conventional symptom checking through a tight bi-directional integration with the electronic medical record (EMR). Conditioned on EMR-derived patient history, our system identifies the patient's chief complaint from a free-text entry and then asks a series of discrete questions to obtain relevant symptomatology. The patient-specific data are used to predict detailed ICD-10-CM codes as well as medication, laboratory, and imaging orders. Patient responses and clinical decision support (CDS) predictions are then inserted back into the EMR. To train the machine learning components of SmartTriage, we employed novel data sets of over 25 million primary care encounters and 1 million patient free-text reason-for-visit entries. These data sets were used to construct: (1) a long short-term memory (LSTM) based patient history representation, (2) a fine-tuned transformer model for chief complaint extraction, (3) a random forest model for question sequencing, and (4) a feed-forward network for CDS predictions. We also present the full production architecture for the pilot deployment of SmartTriage that covers 337 patient chief complaints.
Evaluating robustness of language models for chief complaint extraction from patient-generated text
Nov 15, 2019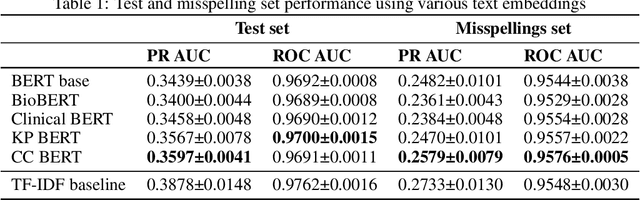
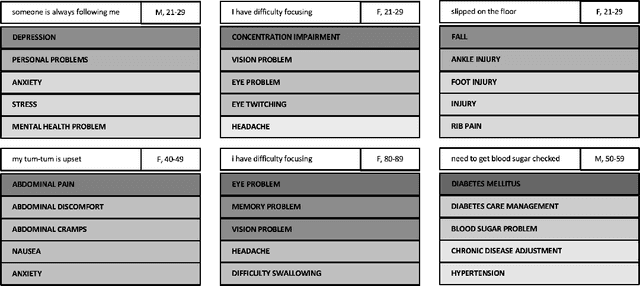
Automated classification of chief complaints from patient-generated text is a critical first step in developing scalable platforms to triage patients without human intervention. In this work, we evaluate several approaches to chief complaint classification using a novel Chief Complaint (CC) Dataset that contains ~200,000 patient-generated reasons-for-visit entries mapped to a set of 795 discrete chief complaints. We examine the use of several fine-tuned bidirectional transformer (BERT) models trained on both unrelated texts as well as on the CC dataset. We contrast this performance with a TF-IDF baseline. Our evaluation has three components: (1) a random test hold-out from the original dataset; (2) a "misspelling set," consisting of a hand-selected subset of the test set, where every entry has at least one misspelling; (3) a separate experimenter-generated free-text set. We find that the TF-IDF model performs significantly better than the strongest BERT-based model on the test (best BERT PR-AUC $0.3597 \pm 0.0041$ vs TF-IDF PR-AUC $0.3878 \pm 0.0148$, $p=7\cdot 10^{-5}$), and is statistically comparable to the misspelling sets (best BERT PR-AUC $0.2579 \pm 0.0079$ vs TF-IDF PR-AUC $0.2733 \pm 0.0130$, $p=0.06$). However, when examining model predictions on experimenter-generated queries, some concerns arise about TF-IDF baseline's robustness. Our results suggest that in certain tasks, simple language embedding baselines may be very performant; however, truly understanding their robustness requires further analysis.