 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeReproducibility of an airway tapering measurement in CT with application to bronchiectasis
Sep 16, 2019



Purpose: This paper proposes a pipeline to acquire a scalar tapering measurement from the carina to the most distal point of an individual airway visible on CT. We show the applicability of using tapering measurements on clinically acquired data by quantifying the reproducibility of the tapering measure. Methods: We generate a spline from the centreline of an airway to measure the area and arclength at contiguous intervals. The tapering measurement is the gradient of the linear regression between area in log space and arclength. The reproducibility of the measure was assessed by analysing different radiation doses, voxel sizes and reconstruction kernel on single timepoint and longitudinal CT scans and by evaluating the effct of airway bifurcations. Results: Using 74 airways from 10 CT scans, we show a statistical difference, p = 3.4 $\times$ 10$^{-4}$ in tapering between healthy airways (n = 35) and those affected by bronchiectasis (n = 39). The difference between the mean of the two populations was 0.011mm$^{-1}$ and the difference between the medians of the two populations was 0.006mm$^{-1}$. The tapering measurement retained a 95\% confidence interval of $\pm$0.005mm$^{-1}$ in a simulated 25 mAs scan and retained a 95% confidence of $\pm$0.005mm$^{-1}$ on simulated CTs up to 1.5 times the original voxel size. Conclusion: We have established an estimate of the precision of the tapering measurement and estimated the effect on precision of simulated voxel size and CT scan dose. We recommend that the scanner calibration be undertaken with the phantoms as described, on the specific CT scanner, radiation dose and reconstruction algorithm that is to be used in any quantitative studies. Our code is available at https://github.com/quan14/AirwayTaperingInCT
* 55 pages, 18 figures, The manuscript was originally published in Journal of Medical Imaging
Tapering Analysis of Airways with Bronchiectasis
Sep 14, 2019Bronchiectasis is the permanent dilation of airways. Patients with the disease can suffer recurrent exacerbations, reducing their quality of life. The gold standard to diagnose and monitor bronchiectasis is accomplished by inspection of chest computed tomography (CT) scans. A clinician examines the broncho-arterial ratio to determine if an airway is brochiectatic. The visual analysis assumes the blood vessel diameter remains constant, although this assumption is disputed in the literature. We propose a simple measurement of tapering along the airways to diagnose and monitor bronchiectasis. To this end, we constructed a pipeline to measure the cross-sectional area along the airways at contiguous intervals, starting from the carina to the most distal point observable. Using a phantom with calibrated 3D printed structures, the precision and accuracy of our algorithm extends to the sub voxel level. The tapering measurement is robust to bifurcations along the airway and was applied to chest CT images acquired in clinical practice. The result is a statistical difference in tapering rate between airways with bronchiectasis and controls. Our code is available at https://github.com/quan14/AirwayTaperingInCT.
* 12 pages, 7 figures. Previously submitted for SPIE Medical Imaging, 2018, Houston, Texas, United States
Uncertainty in multitask learning: joint representations for probabilistic MR-only radiotherapy planning
Jun 18, 2018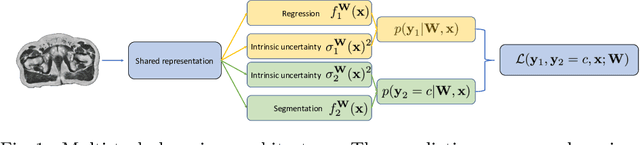
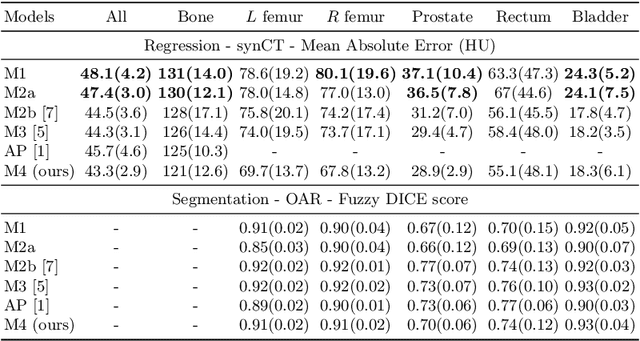
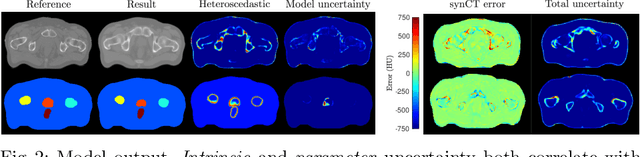
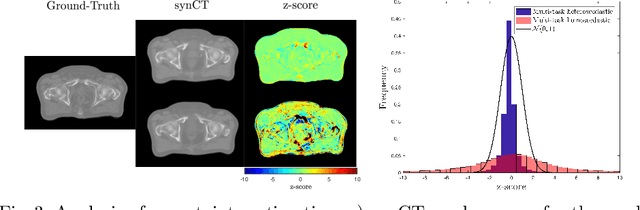
Multi-task neural network architectures provide a mechanism that jointly integrates information from distinct sources. It is ideal in the context of MR-only radiotherapy planning as it can jointly regress a synthetic CT (synCT) scan and segment organs-at-risk (OAR) from MRI. We propose a probabilistic multi-task network that estimates: 1) intrinsic uncertainty through a heteroscedastic noise model for spatially-adaptive task loss weighting and 2) parameter uncertainty through approximate Bayesian inference. This allows sampling of multiple segmentations and synCTs that share their network representation. We test our model on prostate cancer scans and show that it produces more accurate and consistent synCTs with a better estimation in the variance of the errors, state of the art results in OAR segmentation and a methodology for quality assurance in radiotherapy treatment planning.
Augmented Reality needle ablation guidance tool for Irreversible Electroporation in the pancreas
Feb 09, 2018Irreversible electroporation (IRE) is a soft tissue ablation technique suitable for treatment of inoperable tumours in the pancreas. The process involves applying a high voltage electric field to the tissue containing the mass using needle electrodes, leaving cancerous cells irreversibly damaged and vulnerable to apoptosis. Efficacy of the treatment depends heavily on the accuracy of needle placement and requires a high degree of skill from the operator. In this paper, we describe an Augmented Reality (AR) system designed to overcome the challenges associated with planning and guiding the needle insertion process. Our solution, based on the HoloLens (Microsoft, USA) platform, tracks the position of the headset, needle electrodes and ultrasound (US) probe in space. The proof of concept implementation of the system uses this tracking data to render real-time holographic guides on the HoloLens, giving the user insight into the current progress of needle insertion and an indication of the target needle trajectory. The operator's field of view is augmented using visual guides and real-time US feed rendered on a holographic plane, eliminating the need to consult external monitors. Based on these early prototypes, we are aiming to develop a system that will lower the skill level required for IRE while increasing overall accuracy of needle insertion and, hence, the likelihood of successful treatment.
Computer-assisted polyp matching between optical colonoscopy and CT colonography: a phantom study
Jan 15, 2015Potentially precancerous polyps detected with CT colonography (CTC) need to be removed subsequently, using an optical colonoscope (OC). Due to large colonic deformations induced by the colonoscope, even very experienced colonoscopists find it difficult to pinpoint the exact location of the colonoscope tip in relation to polyps reported on CTC. This can cause unduly prolonged OC examinations that are stressful for the patient, colonoscopist and supporting staff. We developed a method, based on monocular 3D reconstruction from OC images, that automatically matches polyps observed in OC with polyps reported on prior CTC. A matching cost is computed, using rigid point-based registration between surface point clouds extracted from both modalities. A 3D printed and painted phantom of a 25 cm long transverse colon segment was used to validate the method on two medium sized polyps. Results indicate that the matching cost is smaller at the correct corresponding polyp between OC and CTC: the value is 3.9 times higher at the incorrect polyp, comparing the correct match between polyps to the incorrect match. Furthermore, we evaluate the matching of the reconstructed polyp from OC with other colonic endoluminal surface structures such as haustral folds and show that there is a minimum at the correct polyp from CTC. Automated matching between polyps observed at OC and prior CTC would facilitate the biopsy or removal of true-positive pathology or exclusion of false-positive CTC findings, and would reduce colonoscopy false-negative (missed) polyps. Ultimately, such a method might reduce healthcare costs, patient inconvenience and discomfort.
* This paper was presented at the SPIE Medical Imaging 2014 conference
Numerical Methods for Coupled Reconstruction and Registration in Digital Breast Tomosynthesis
Jul 23, 2013



Digital Breast Tomosynthesis (DBT) provides an insight into the fine details of normal fibroglandular tissues and abnormal lesions by reconstructing a pseudo-3D image of the breast. In this respect, DBT overcomes a major limitation of conventional X-ray mammography by reducing the confounding effects caused by the superposition of breast tissue. In a breast cancer screening or diagnostic context, a radiologist is interested in detecting change, which might be indicative of malignant disease. To help automate this task image registration is required to establish spatial correspondence between time points. Typically, images, such as MRI or CT, are first reconstructed and then registered. This approach can be effective if reconstructing using a complete set of data. However, for ill-posed, limited-angle problems such as DBT, estimating the deformation is complicated by the significant artefacts associated with the reconstruction, leading to severe inaccuracies in the registration. This paper presents a mathematical framework, which couples the two tasks and jointly estimates both image intensities and the parameters of a transformation. We evaluate our methods using various computational digital phantoms, uncompressed breast MR images, and in-vivo DBT simulations. Firstly, we compare both iterative and simultaneous methods to the conventional, sequential method using an affine transformation model. We show that jointly estimating image intensities and parametric transformations gives superior results with respect to reconstruction fidelity and registration accuracy. Also, we incorporate a non-rigid B-spline transformation model into our simultaneous method. The results demonstrate a visually plausible recovery of the deformation with preservation of the reconstruction fidelity.