 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to Edge3D Whole Brain Segmentation using Spatially Localized Atlas Network Tiles
Mar 28, 2019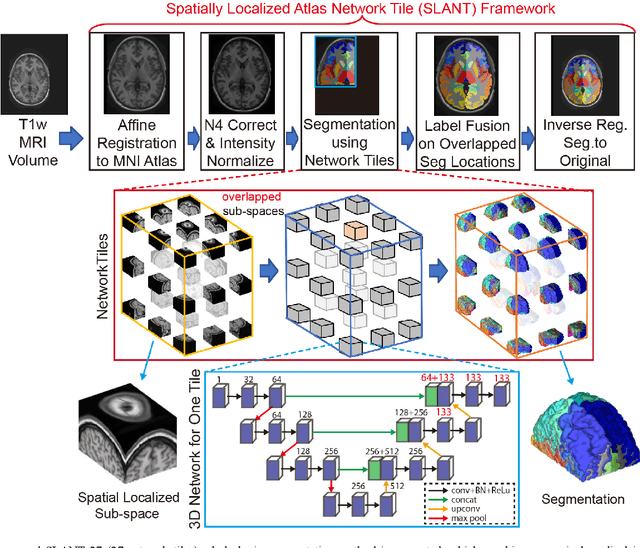
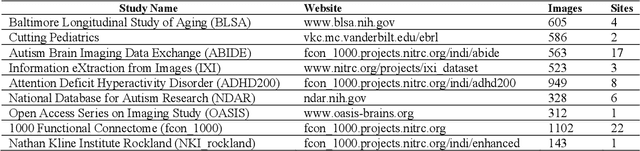
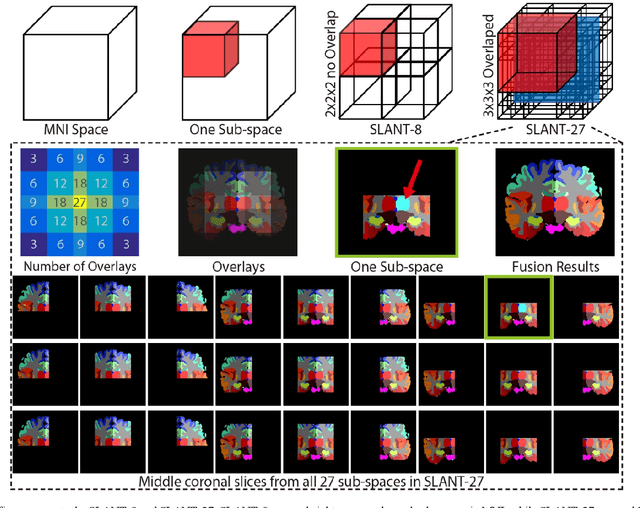
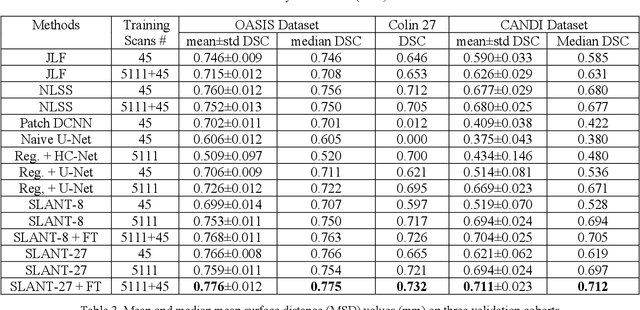
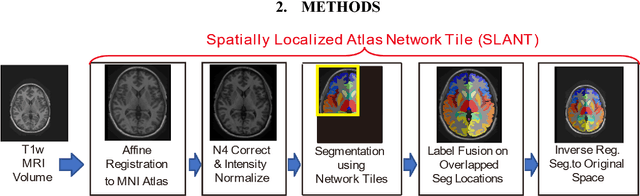
Detailed whole brain segmentation is an essential quantitative technique, which provides a non-invasive way of measuring brain regions from a structural magnetic resonance imaging (MRI). Recently, deep convolution neural network (CNN) has been applied to whole brain segmentation. However, restricted by current GPU memory, 2D based methods, downsampling based 3D CNN methods, and patch-based high-resolution 3D CNN methods have been the de facto standard solutions. 3D patch-based high resolution methods typically yield superior performance among CNN approaches on detailed whole brain segmentation (>100 labels), however, whose performance are still commonly inferior compared with multi-atlas segmentation methods (MAS) due to the following challenges: (1) a single network is typically used to learn both spatial and contextual information for the patches, (2) limited manually traced whole brain volumes are available (typically less than 50) for training a network. In this work, we propose the spatially localized atlas network tiles (SLANT) method to distribute multiple independent 3D fully convolutional networks (FCN) for high-resolution whole brain segmentation. To address the first challenge, multiple spatially distributed networks were used in the SLANT method, in which each network learned contextual information for a fixed spatial location. To address the second challenge, auxiliary labels on 5111 initially unlabeled scans were created by multi-atlas segmentation for training. Since the method integrated multiple traditional medical image processing methods with deep learning, we developed a containerized pipeline to deploy the end-to-end solution. From the results, the proposed method achieved superior performance compared with multi-atlas segmentation methods, while reducing the computational time from >30 hours to 15 minutes (https://github.com/MASILab/SLANTbrainSeg).
Lung Cancer Detection using Co-learning from Chest CT Images and Clinical Demographics
Feb 21, 2019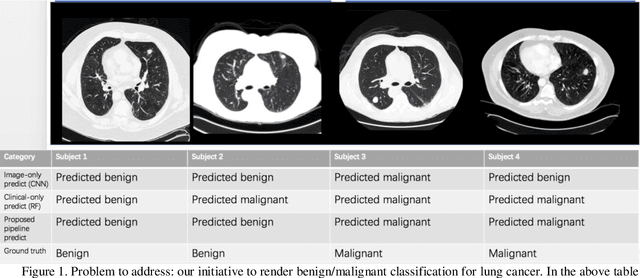
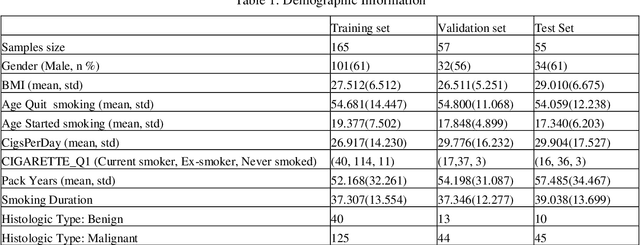
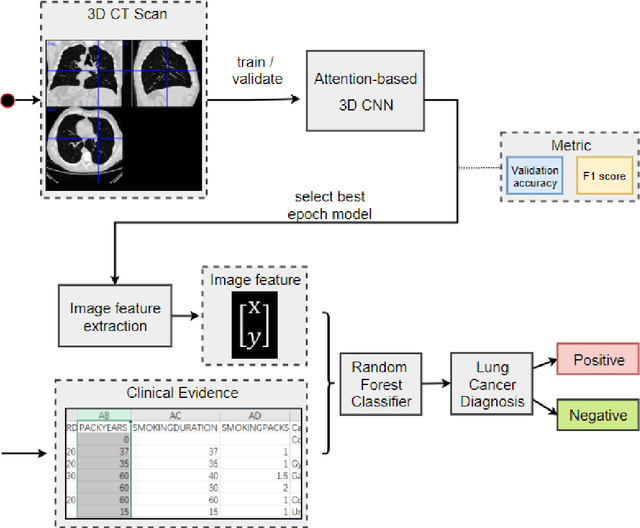
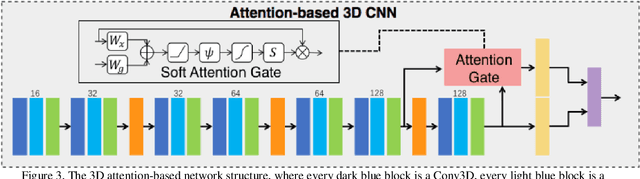
Early detection of lung cancer is essential in reducing mortality. Recent studies have demonstrated the clinical utility of low-dose computed tomography (CT) to detect lung cancer among individuals selected based on very limited clinical information. However, this strategy yields high false positive rates, which can lead to unnecessary and potentially harmful procedures. To address such challenges, we established a pipeline that co-learns from detailed clinical demographics and 3D CT images. Toward this end, we leveraged data from the Consortium for Molecular and Cellular Characterization of Screen-Detected Lesions (MCL), which focuses on early detection of lung cancer. A 3D attention-based deep convolutional neural net (DCNN) is proposed to identify lung cancer from the chest CT scan without prior anatomical location of the suspicious nodule. To improve upon the non-invasive discrimination between benign and malignant, we applied a random forest classifier to a dataset integrating clinical information to imaging data. The results show that the AUC obtained from clinical demographics alone was 0.635 while the attention network alone reached an accuracy of 0.687. In contrast when applying our proposed pipeline integrating clinical and imaging variables, we reached an AUC of 0.787 on the testing dataset. The proposed network both efficiently captures anatomical information for classification and also generates attention maps that explain the features that drive performance.
Reproducibility Evaluation of SLANT Whole Brain Segmentation Across Clinical Magnetic Resonance Imaging Protocols
Jan 07, 2019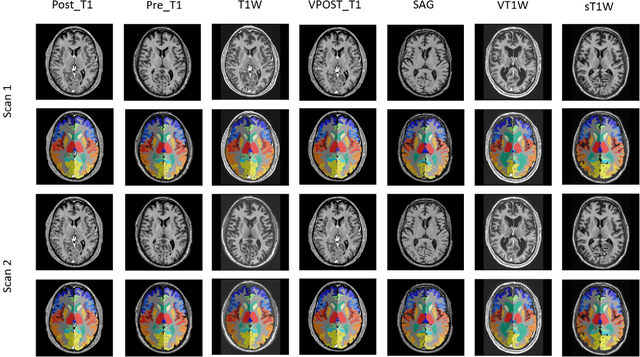
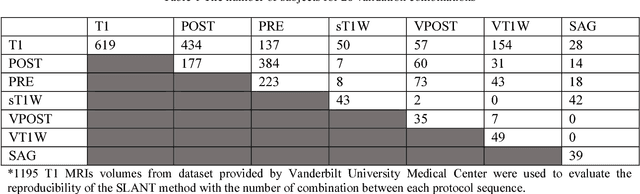

Whole brain segmentation on structural magnetic resonance imaging (MRI) is essential for understanding neuroanatomical-functional relationships. Traditionally, multi-atlas segmentation has been regarded as the standard method for whole brain segmentation. In past few years, deep convolutional neural network (DCNN) segmentation methods have demonstrated their advantages in both accuracy and computational efficiency. Recently, we proposed the spatially localized atlas network tiles (SLANT) method, which is able to segment a 3D MRI brain scan into 132 anatomical regions. Commonly, DCNN segmentation methods yield inferior performance under external validations, especially when the testing patterns were not presented in the training cohorts. Recently, we obtained a clinically acquired, multi-sequence MRI brain cohort with 1480 clinically acquired, de-identified brain MRI scans on 395 patients using seven different MRI protocols. Moreover, each subject has at least two scans from different MRI protocols. Herein, we assess the SLANT method's intra- and inter-protocol reproducibility. SLANT achieved less than 0.05 coefficient of variation (CV) for intra-protocol experiments and less than 0.15 CV for inter-protocol experiments. The results show that the SLANT method achieved high intra- and inter- protocol reproducibility.