 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeVisual-Haptic Model Mediated Teleoperation for Remote Ultrasound
Feb 11, 2025Tele-ultrasound has the potential greatly to improve health equity for countless remote communities. However, practical scenarios involve potentially large time delays which cause current implementations of telerobotic ultrasound (US) to fail. Using a local model of the remote environment to provide haptics to the expert operator can decrease teleoperation instability, but the delayed visual feedback remains problematic. This paper introduces a robotic tele-US system in which the local model is not only haptic, but also visual, by re-slicing and rendering a pre-acquired US sweep in real time to provide the operator a preview of what the delayed image will resemble. A prototype system is presented and tested with 15 volunteer operators. It is found that visual-haptic model-mediated teleoperation (MMT) compensates completely for time delays up to 1000 ms round trip in terms of operator effort and completion time while conventional MMT does not. Visual-haptic MMT also significantly outperforms MMT for longer time delays in terms of motion accuracy and force control. This proof-of-concept study suggests that visual-haptic MMT may facilitate remote robotic tele-US.
PRO-TIP: Phantom for RObust automatic ultrasound calibration by TIP detection
Jun 13, 2022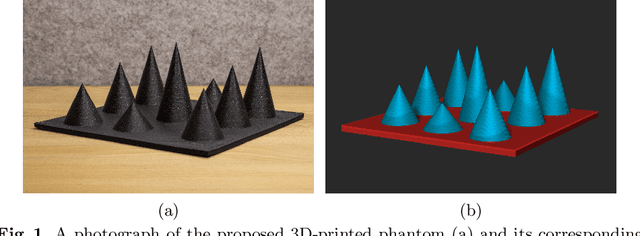
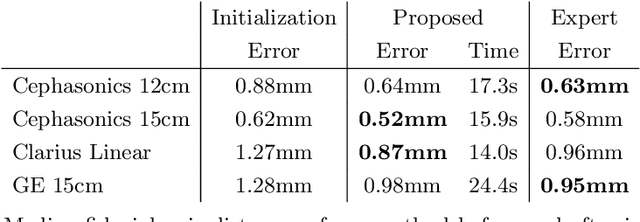
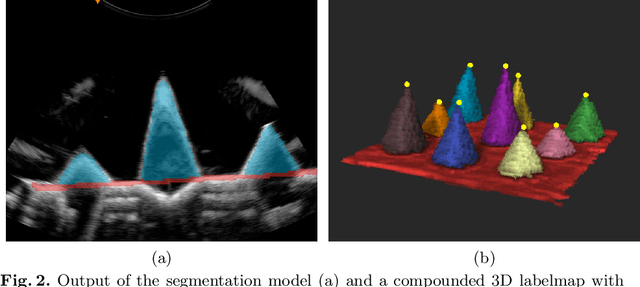
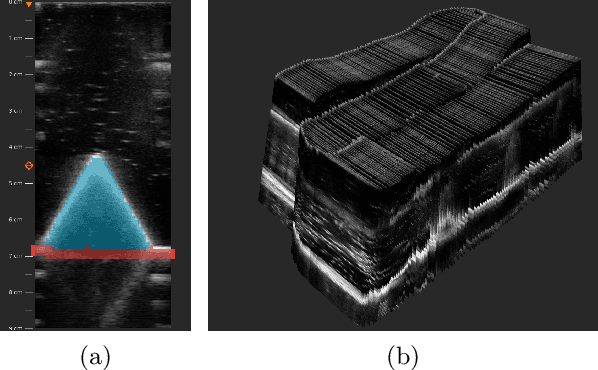
We propose a novel method to automatically calibrate tracked ultrasound probes. To this end we design a custom phantom consisting of nine cones with different heights. The tips are used as key points to be matched between multiple sweeps. We extract them using a convolutional neural network to segment the cones in every ultrasound frame and then track them across the sweep. The calibration is robustly estimated using RANSAC and later refined employing image based techniques. Our phantom can be 3D-printed and offers many advantages over state-of-the-art methods. The phantom design and algorithm code are freely available online. Since our phantom does not require a tracking target on itself, ease of use is improved over currently used techniques. The fully automatic method generalizes to new probes and different vendors, as shown in our experiments. Our approach produces results comparable to calibrations obtained by a domain expert.
Rethinking Ultrasound Augmentation: A Physics-Inspired Approach
May 05, 2021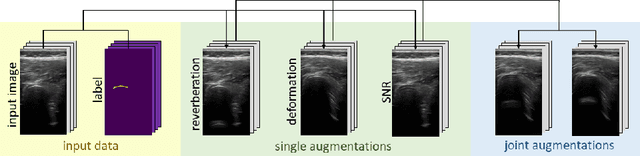
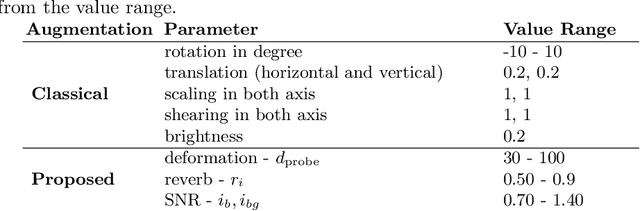
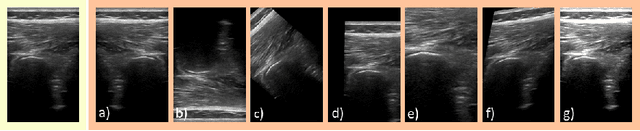
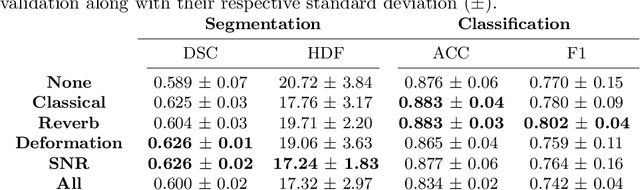
Medical Ultrasound (US), despite its wide use, is characterized by artifacts and operator dependency. Those attributes hinder the gathering and utilization of US datasets for the training of Deep Neural Networks used for Computer-Assisted Intervention Systems. Data augmentation is commonly used to enhance model generalization and performance. However, common data augmentation techniques, such as affine transformations do not align with the physics of US and, when used carelessly can lead to unrealistic US images. To this end, we propose a set of physics-inspired transformations, including deformation, reverb and Signal-to-Noise Ratio, that we apply on US B-mode images for data augmentation. We evaluate our method on a new spine US dataset for the tasks of bone segmentation and classification.
Ultrasound-Guided Robotic Navigation with Deep Reinforcement Learning
Apr 07, 2020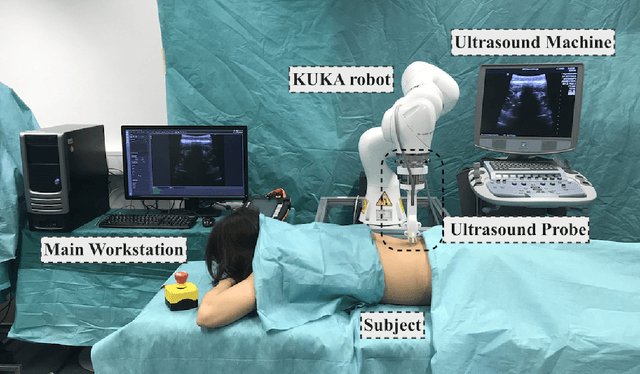
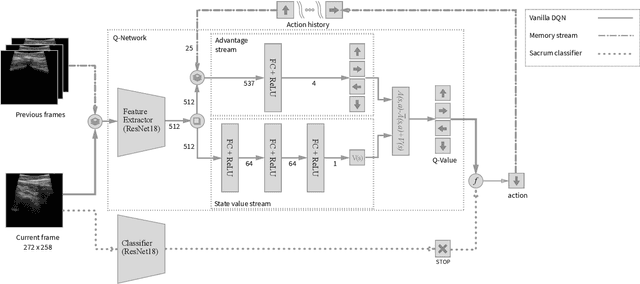
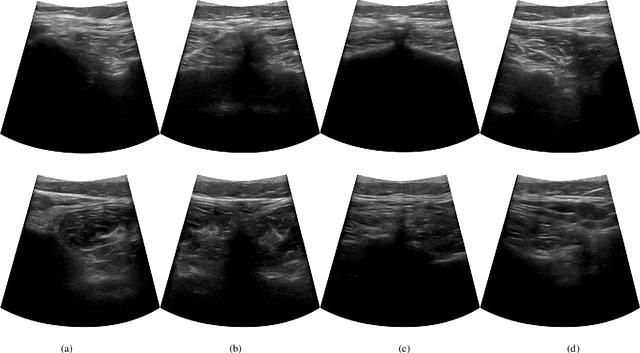
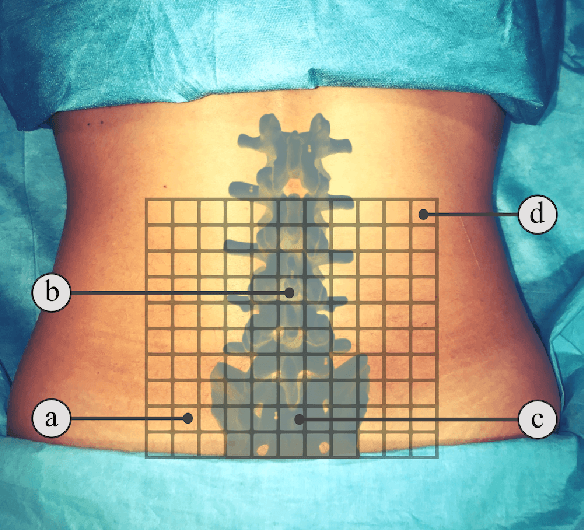
In this paper we introduce the first reinforcement learning (RL) based robotic navigation method which utilizes ultrasound (US) images as an input. Our approach combines state-of-the-art RL techniques, specifically deep Q-networks (DQN) with memory buffers and a binary classifier for deciding when to terminate the task. Our method is trained and evaluated on an in-house collected data-set of 34 volunteers and when compared to pure RL and supervised learning (SL) techniques, it performs substantially better, which highlights the suitability of RL navigation for US-guided procedures. When testing our proposed model, we obtained a 82.91% chance of navigating correctly to the sacrum from 165 different starting positions on 5 different unseen simulated environments.
Force-Ultrasound Fusion: Bringing Spine Robotic-US to the Next "Level"
Feb 26, 2020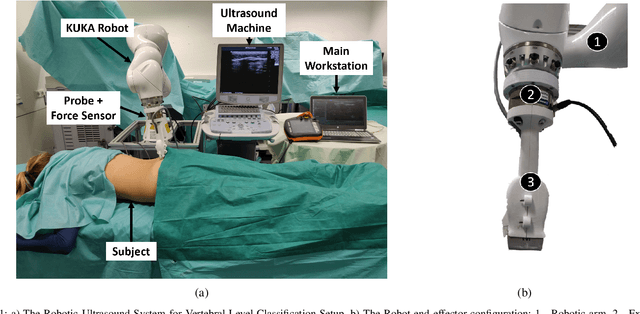

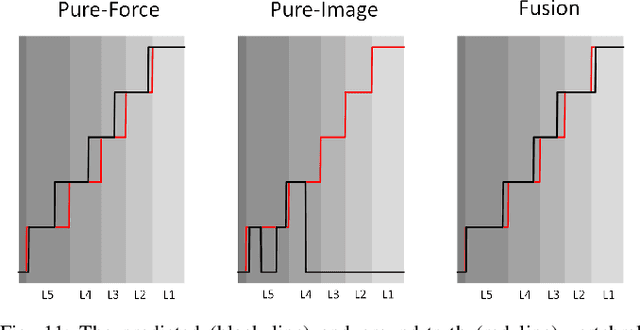
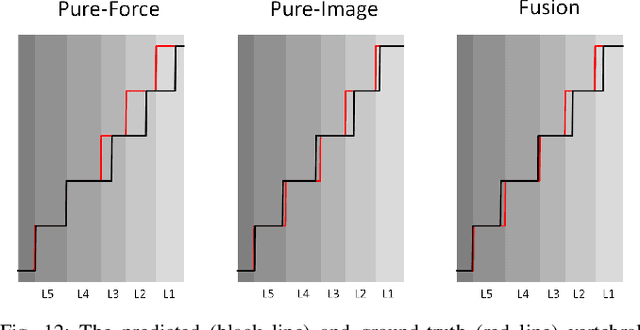
Spine injections are commonly performed in several clinical procedures. The localization of the target vertebral level (i.e. the position of a vertebra in a spine) is typically done by back palpation or under X-ray guidance, yielding either higher chances of procedure failure or exposure to ionizing radiation. Preliminary studies have been conducted in the literature, suggesting that ultrasound imaging may be a precise and safe alternative to X-ray for spine level detection. However, ultrasound data are noisy and complicated to interpret. In this study, a robotic-ultrasound approach for automatic vertebral level detection is introduced. The method relies on the fusion of ultrasound and force data, thus providing both "tactile" and visual feedback during the procedure, which results in higher performances in presence of data corruption. A robotic arm automatically scans the volunteer's back along the spine by using force-ultrasound data to locate vertebral levels. The occurrences of vertebral levels are visible on the force trace as peaks, which are enhanced by properly controlling the force applied by the robot on the patient back. Ultrasound data are processed with a Deep Learning method to extract a 1D signal modelling the probabilities of having a vertebra at each location along the spine. Processed force and ultrasound data are fused using a 1D Convolutional Network to compute the location of the vertebral levels. The method is compared to pure image and pure force-based methods for vertebral level counting, showing improved performance. In particular, the fusion method is able to correctly classify 100% of the vertebral levels in the test set, while pure image and pure force-based method could only classify 80% and 90% vertebrae, respectively. The potential of the proposed method is evaluated in an exemplary simulated clinical application.