 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeEvaluation of General Large Language Models in Contextually Assessing Semantic Concepts Extracted from Adult Critical Care Electronic Health Record Notes
Jan 24, 2024The field of healthcare has increasingly turned its focus towards Large Language Models (LLMs) due to their remarkable performance. However, their performance in actual clinical applications has been underexplored. Traditional evaluations based on question-answering tasks don't fully capture the nuanced contexts. This gap highlights the need for more in-depth and practical assessments of LLMs in real-world healthcare settings. Objective: We sought to evaluate the performance of LLMs in the complex clinical context of adult critical care medicine using systematic and comprehensible analytic methods, including clinician annotation and adjudication. Methods: We investigated the performance of three general LLMs in understanding and processing real-world clinical notes. Concepts from 150 clinical notes were identified by MetaMap and then labeled by 9 clinicians. Each LLM's proficiency was evaluated by identifying the temporality and negation of these concepts using different prompts for an in-depth analysis. Results: GPT-4 showed overall superior performance compared to other LLMs. In contrast, both GPT-3.5 and text-davinci-003 exhibit enhanced performance when the appropriate prompting strategies are employed. The GPT family models have demonstrated considerable efficiency, evidenced by their cost-effectiveness and time-saving capabilities. Conclusion: A comprehensive qualitative performance evaluation framework for LLMs is developed and operationalized. This framework goes beyond singular performance aspects. With expert annotations, this methodology not only validates LLMs' capabilities in processing complex medical data but also establishes a benchmark for future LLM evaluations across specialized domains.
Weakly Supervised Classification of Vital Sign Alerts as Real or Artifact
Jun 18, 2022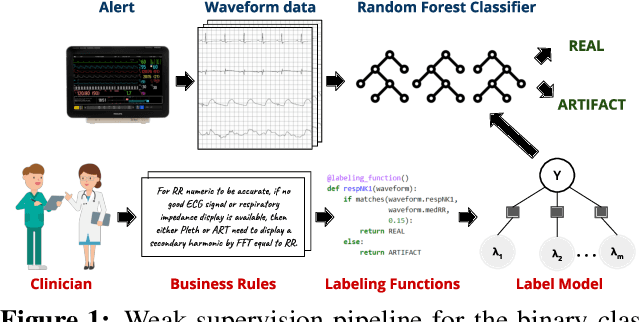


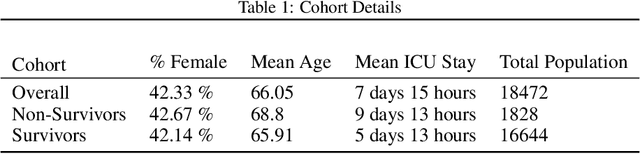
A significant proportion of clinical physiologic monitoring alarms are false. This often leads to alarm fatigue in clinical personnel, inevitably compromising patient safety. To combat this issue, researchers have attempted to build Machine Learning (ML) models capable of accurately adjudicating Vital Sign (VS) alerts raised at the bedside of hemodynamically monitored patients as real or artifact. Previous studies have utilized supervised ML techniques that require substantial amounts of hand-labeled data. However, manually harvesting such data can be costly, time-consuming, and mundane, and is a key factor limiting the widespread adoption of ML in healthcare (HC). Instead, we explore the use of multiple, individually imperfect heuristics to automatically assign probabilistic labels to unlabeled training data using weak supervision. Our weakly supervised models perform competitively with traditional supervised techniques and require less involvement from domain experts, demonstrating their use as efficient and practical alternatives to supervised learning in HC applications of ML.
Deep Normed Embeddings for Patient Representation
Apr 12, 2022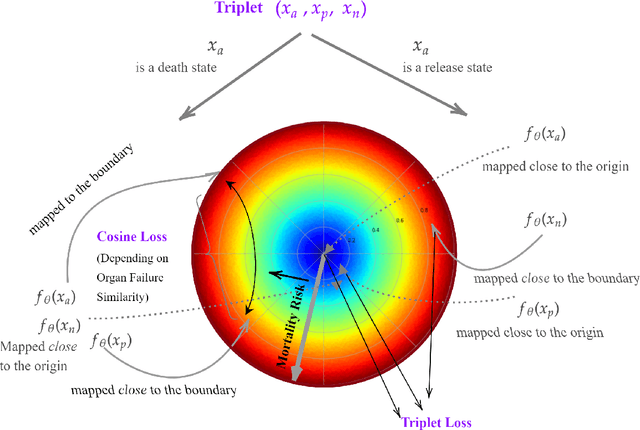

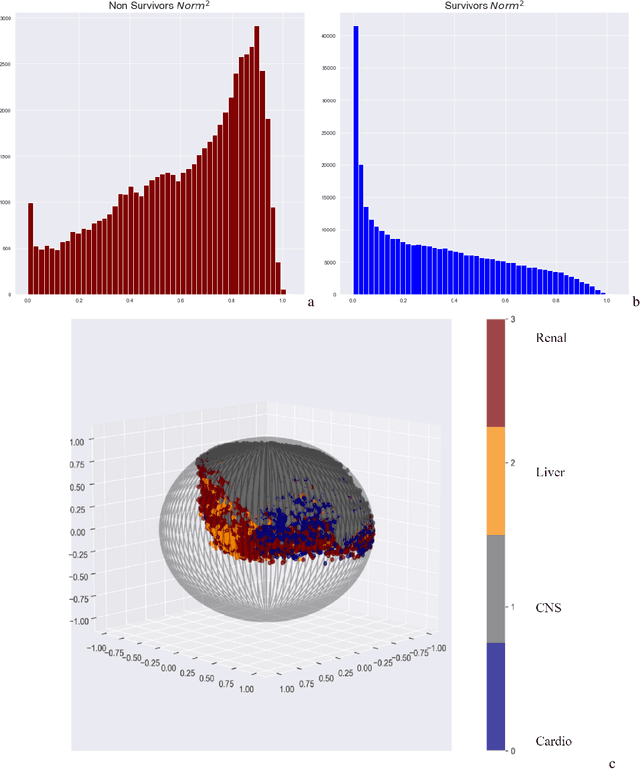

We introduce a novel contrastive representation learning objective and a training scheme for clinical time series. Specifically, we project high dimensional E.H.R. data to a closed unit ball of low dimension, encoding geometric priors so that the origin represents an idealized perfect health state and the euclidean norm is associated with the patient's mortality risk. Moreover, using septic patients as an example, we show how we could learn to associate the angle between two vectors with the different organ system failures, thereby, learning a compact representation which is indicative of both mortality risk and specific organ failure. We show how the learned embedding can be used for online patient monitoring, supplement clinicians and improve performance of downstream machine learning tasks. This work was partially motivated from the desire and the need to introduce a systematic way of defining intermediate rewards for Reinforcement Learning in critical care medicine. Hence, we also show how such a design in terms of the learned embedding can result in qualitatively different policies and value distributions, as compared with using only terminal rewards.
Unifying Cardiovascular Modelling with Deep Reinforcement Learning for Uncertainty Aware Control of Sepsis Treatment
Feb 02, 2021


Sepsis is the leading cause of mortality in the ICU, responsible for 6% of all hospitalizations and 35% of all in-hospital deaths in USA. However, there is no universally agreed upon strategy for vasopressor and fluid administration. It has also been observed that different patients respond differently to treatment, highlighting the need for individualized treatment. Vasopressors and fluids are administrated with specific effects to cardiovascular physiology in mind and medical research has suggested that physiologic, hemodynamically guided, approaches to treatment. Thus we propose a novel approach, exploiting and unifying complementary strengths of Mathematical Modelling, Deep Learning, Reinforcement Learning and Uncertainty Quantification, to learn individualized, safe, and uncertainty aware treatment strategies. We first infer patient-specific, dynamic cardiovascular states using a novel physiology-driven recurrent neural network trained in an unsupervised manner. This information, along with a learned low dimensional representation of the patient's lab history and observable data, is then used to derive value distributions using Batch Distributional Reinforcement Learning. Moreover in a safety critical domain it is essential to know what our agent does and does not know, for this we also quantify the model uncertainty associated with each patient state and action, and propose a general framework for uncertainty aware, interpretable treatment policies. This framework can be tweaked easily, to reflect a clinician's own confidence of the framework, and can be easily modified to factor in human expert opinion, whenever it's accessible. Using representative patients and a validation cohort, we show that our method has learned physiologically interpretable generalizable policies.