 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeObserving the unobserved confounding through its effects: toward randomized trial-like estimates from real-world survival data
Apr 13, 2026Background: Randomized controlled trials (RCTs) are costly, time-consuming, and often infeasible, while treatment-effect estimation from observational data is limited by unobserved confounding. Methods: We developed a three-step framework to address unobserved confounding in observational survival data. First, we infer a latent prognostic factor (U) from restricted mean survival time (RMST) discrepancies between patients with similar observed factors, the same treatment, and divergent outcomes, leveraging the idea that the aggregate effect of unmeasured factors can be inferred even if individual factors cannot. Second, we balance U with observed baseline covariates using prognostic matching, entropy balancing, or inverse probability of treatment weighting. Third, we apply multivariable survival analysis to estimate hazard ratios (HRs). We evaluated the framework in three observational cohorts with RCT benchmarks, two RCT cohorts, and six multicenter observational cohorts. Results: In three observational cohorts (nine comparisons), balancing U improved agreement with trial HRs in all cases; in the strongest settings, it reduced absolute log-HR error by approximately ten-fold versus using observed covariates alone (mean reduction 0.344; p=0.001). In two RCT cohorts, U was balanced across arms (most SMDs <0.1) and adjustment had minimal impact on log-HRs (mean absolute change 0.08). Across six multicenter cohorts, balancing U within centers reduced cross-center dispersion in chemotherapy log-HR estimates (mean reduction 0.147; p=0.016); when populations were directly balanced across centers to account for case-mix differences, cross-center survival differences were narrowed in 75%-100% of comparisons. Conclusions: Inferring and balancing a latent prognostic signal may reduce unobserved confounding and improve treatment-effect estimation from real-world data.
Early Warning Index for Patient Deteriorations in Hospitals
Dec 16, 2025

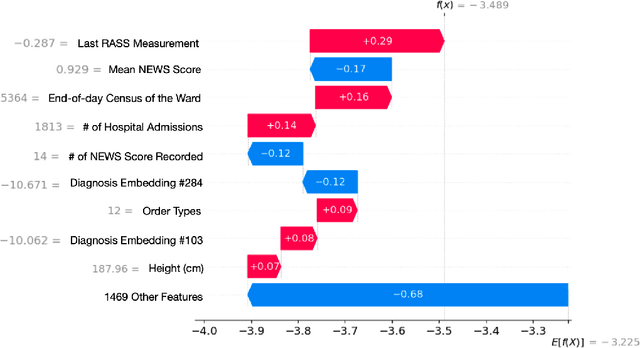

Hospitals lack automated systems to harness the growing volume of heterogeneous clinical and operational data to effectively forecast critical events. Early identification of patients at risk for deterioration is essential not only for patient care quality monitoring but also for physician care management. However, translating varied data streams into accurate and interpretable risk assessments poses significant challenges due to inconsistent data formats. We develop a multimodal machine learning framework, the Early Warning Index (EWI), to predict the aggregate risk of ICU admission, emergency response team dispatch, and mortality. Key to EWI's design is a human-in-the-loop process: clinicians help determine alert thresholds and interpret model outputs, which are enhanced by explainable outputs using Shapley Additive exPlanations (SHAP) to highlight clinical and operational factors (e.g., scheduled surgeries, ward census) driving each patient's risk. We deploy EWI in a hospital dashboard that stratifies patients into three risk tiers. Using a dataset of 18,633 unique patients at a large U.S. hospital, our approach automatically extracts features from both structured and unstructured electronic health record (EHR) data and achieves C-statistics of 0.796. It is currently used as a triage tool for proactively managing at-risk patients. The proposed approach saves physicians valuable time by automatically sorting patients of varying risk levels, allowing them to concentrate on patient care rather than sifting through complex EHR data. By further pinpointing specific risk drivers, the proposed model provides data-informed adjustments to caregiver scheduling and allocation of critical resources. As a result, clinicians and administrators can avert downstream complications, including costly procedures or high readmission rates and improve overall patient flow.
An Interpretable AI Tool for SAVR vs TAVR in Low to Intermediate Risk Patients with Severe Aortic Stenosis
Dec 11, 2025Background. Treatment selection for low to intermediate risk patients with severe aortic stenosis between surgical (SAVR) and transcatheter (TAVR) aortic valve replacement remains variable in clinical practice, driven by patient heterogeneity and institutional preferences. While existing models predict postprocedural risk, there is a lack of interpretable, individualized treatment recommendations that directly optimize long-term outcomes. Methods. We introduce an interpretable prescriptive framework that integrates prognostic matching, counterfactual outcome modeling, and an Optimal Policy Tree (OPT) to recommend the treatment minimizing expected 5-year mortality. Using data from Hartford Hospital and St. Vincent's Hospital, we emulate randomization via prognostic matching and sample weighting and estimate counterfactual mortality under both SAVR and TAVR. The policy model, trained on these counterfactual predictions, partitions patients into clinically coherent subgroups and prescribes the treatment associated with lower estimated risk. Findings. If the OPT prescriptions are applied, counterfactual evaluation showed an estimated reduction in 5-year mortality of 20.3\% in Hartford and 13.8\% in St. Vincent's relative to real-life prescriptions, showing promising generalizability to unseen data from a different institution. The learned decision boundaries aligned with real-world outcomes and clinical observations. Interpretation. Our interpretable prescriptive framework is, to the best of our knowledge, the first to provide transparent, data-driven recommendations for TAVR versus SAVR that improve estimated long-term outcomes both in an internal and external cohort, while remaining clinically grounded and contributing toward a more systematic and evidence-based approach to precision medicine in structural heart disease.
Detection and Localization of Subdural Hematoma Using Deep Learning on Computed Tomography
Dec 10, 2025Background. Subdural hematoma (SDH) is a common neurosurgical emergency, with increasing incidence in aging populations. Rapid and accurate identification is essential to guide timely intervention, yet existing automated tools focus primarily on detection and provide limited interpretability or spatial localization. There remains a need for transparent, high-performing systems that integrate multimodal clinical and imaging information to support real-time decision-making. Methods. We developed a multimodal deep-learning framework that integrates structured clinical variables, a 3D convolutional neural network trained on CT volumes, and a transformer-enhanced 2D segmentation model for SDH detection and localization. Using 25,315 head CT studies from Hartford HealthCare (2015--2024), of which 3,774 (14.9\%) contained clinician-confirmed SDH, tabular models were trained on demographics, comorbidities, medications, and laboratory results. Imaging models were trained to detect SDH and generate voxel-level probability maps. A greedy ensemble strategy combined complementary predictors. Findings. Clinical variables alone provided modest discriminatory power (AUC 0.75). Convolutional models trained on CT volumes and segmentation-derived maps achieved substantially higher accuracy (AUCs 0.922 and 0.926). The multimodal ensemble integrating all components achieved the best overall performance (AUC 0.9407; 95\% CI, 0.930--0.951) and produced anatomically meaningful localization maps consistent with known SDH patterns. Interpretation. This multimodal, interpretable framework provides rapid and accurate SDH detection and localization, achieving high detection performance and offering transparent, anatomically grounded outputs. Integration into radiology workflows could streamline triage, reduce time to intervention, and improve consistency in SDH management.
Towards Optimal Valve Prescription for Transcatheter Aortic Valve Replacement (TAVR) Surgery: A Machine Learning Approach
Dec 09, 2025Transcatheter Aortic Valve Replacement (TAVR) has emerged as a minimally invasive treatment option for patients with severe aortic stenosis, a life-threatening cardiovascular condition. Multiple transcatheter heart valves (THV) have been approved for use in TAVR, but current guidelines regarding valve type prescription remain an active topic of debate. We propose a data-driven clinical support tool to identify the optimal valve type with the objective of minimizing the risk of permanent pacemaker implantation (PPI), a predominant postoperative complication. We synthesize a novel dataset that combines U.S. and Greek patient populations and integrates three distinct data sources (patient demographics, computed tomography scans, echocardiograms) while harmonizing differences in each country's record system. We introduce a leaf-level analysis to leverage population heterogeneity and avoid benchmarking against uncertain counterfactual risk estimates. The final prescriptive model shows a reduction in PPI rates of 26% and 16% compared with the current standard of care in our internal U.S. population and external Greek validation cohort, respectively. To the best of our knowledge, this work represents the first unified, personalized prescription strategy for THV selection in TAVR.
Adaptive Forests For Classification
Oct 27, 2025Random Forests (RF) and Extreme Gradient Boosting (XGBoost) are two of the most widely used and highly performing classification and regression models. They aggregate equally weighted CART trees, generated randomly in RF or sequentially in XGBoost. In this paper, we propose Adaptive Forests (AF), a novel approach that adaptively selects the weights of the underlying CART models. AF combines (a) the Optimal Predictive-Policy Trees (OP2T) framework to prescribe tailored, input-dependent unequal weights to trees and (b) Mixed Integer Optimization (MIO) to refine weight candidates dynamically, enhancing overall performance. We demonstrate that AF consistently outperforms RF, XGBoost, and other weighted RF in binary and multi-class classification problems over 20+ real-world datasets.
Prescribe-then-Select: Adaptive Policy Selection for Contextual Stochastic Optimization
Sep 09, 2025We address the problem of policy selection in contextual stochastic optimization (CSO), where covariates are available as contextual information and decisions must satisfy hard feasibility constraints. In many CSO settings, multiple candidate policies--arising from different modeling paradigms--exhibit heterogeneous performance across the covariate space, with no single policy uniformly dominating. We propose Prescribe-then-Select (PS), a modular framework that first constructs a library of feasible candidate policies and then learns a meta-policy to select the best policy for the observed covariates. We implement the meta-policy using ensembles of Optimal Policy Trees trained via cross-validation on the training set, making policy choice entirely data-driven. Across two benchmark CSO problems--single-stage newsvendor and two-stage shipment planning--PS consistently outperforms the best single policy in heterogeneous regimes of the covariate space and converges to the dominant policy when such heterogeneity is absent. All the code to reproduce the results can be found at https://anonymous.4open.science/r/Prescribe-then-Select-TMLR.
From Data to Uncertainty Sets: a Machine Learning Approach
Mar 04, 2025



Existing approaches of prescriptive analytics -- where inputs of an optimization model can be predicted by leveraging covariates in a machine learning model -- often attempt to optimize the mean value of an uncertain objective. However, when applied to uncertain constraints, these methods rarely work because satisfying a crucial constraint in expectation may result in a high probability of violation. To remedy this, we leverage robust optimization to protect a constraint against the uncertainty of a machine learning model's output. To do so, we design an uncertainty set based on the model's loss function. Intuitively, this approach attempts to minimize the uncertainty around a prediction. Extending guarantees from the robust optimization literature, we derive strong guarantees on the probability of violation. On synthetic computational experiments, our method requires uncertainty sets with radii up to one order of magnitude smaller than those of other approaches.
Optimal Control of Fluid Restless Multi-armed Bandits: A Machine Learning Approach
Feb 06, 2025



We propose a machine learning approach to the optimal control of fluid restless multi-armed bandits (FRMABs) with state equations that are either affine or quadratic in the state variables. By deriving fundamental properties of FRMAB problems, we design an efficient machine learning based algorithm. Using this algorithm, we solve multiple instances with varying initial states to generate a comprehensive training set. We then learn a state feedback policy using Optimal Classification Trees with hyperplane splits (OCT-H). We test our approach on machine maintenance, epidemic control and fisheries control problems. Our method yields high-quality state feedback policies and achieves a speed-up of up to 26 million times compared to a direct numerical algorithm for fluid problems.
Multimodal Prescriptive Deep Learning
Jan 24, 2025



We introduce a multimodal deep learning framework, Prescriptive Neural Networks (PNNs), that combines ideas from optimization and machine learning, and is, to the best of our knowledge, the first prescriptive method to handle multimodal data. The PNN is a feedforward neural network trained on embeddings to output an outcome-optimizing prescription. In two real-world multimodal datasets, we demonstrate that PNNs prescribe treatments that are able to significantly improve estimated outcomes in transcatheter aortic valve replacement (TAVR) procedures by reducing estimated postoperative complication rates by 32% and in liver trauma injuries by reducing estimated mortality rates by over 40%. In four real-world, unimodal tabular datasets, we demonstrate that PNNs outperform or perform comparably to other well-known, state-of-the-art prescriptive models; importantly, on tabular datasets, we also recover interpretability through knowledge distillation, fitting interpretable Optimal Classification Tree models onto the PNN prescriptions as classification targets, which is critical for many real-world applications. Finally, we demonstrate that our multimodal PNN models achieve stability across randomized data splits comparable to other prescriptive methods and produce realistic prescriptions across the different datasets.