 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeA multi-cohort study on prediction of acute brain dysfunction states using selective state space models
Mar 11, 2024

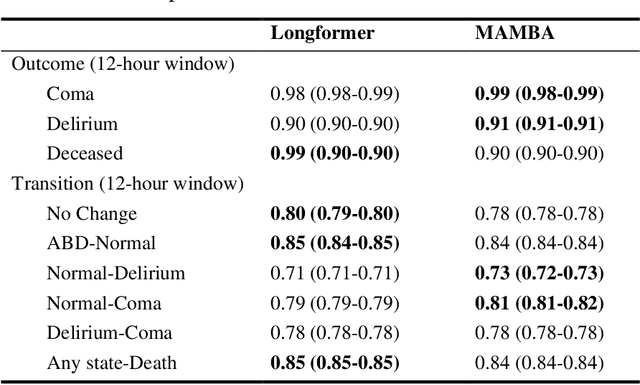

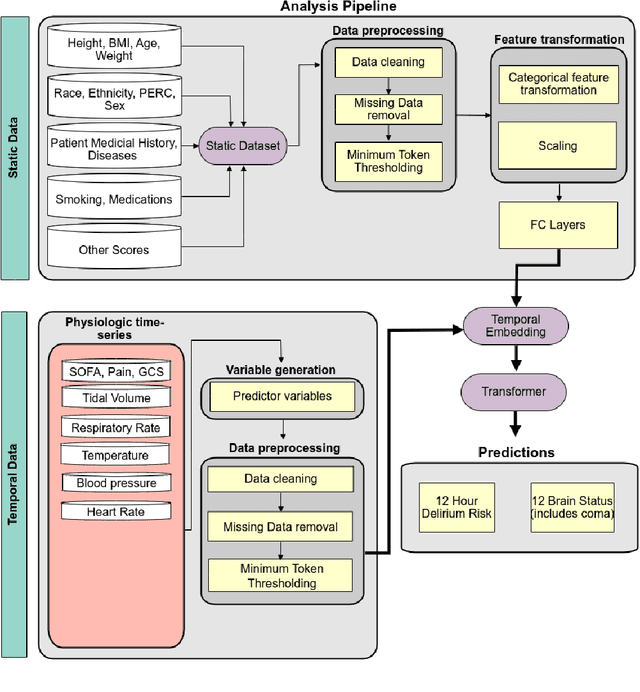
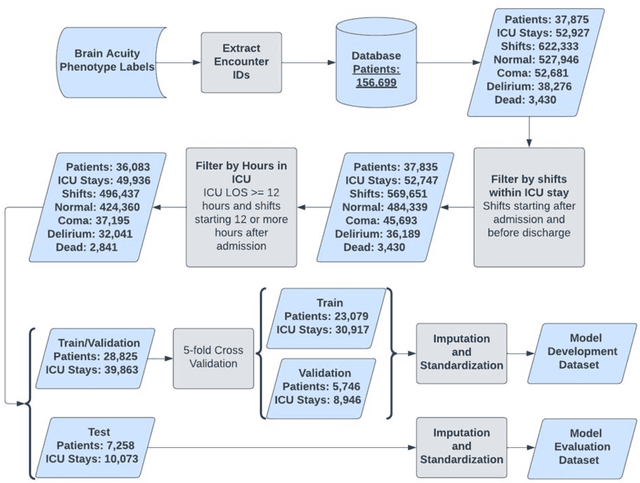
Assessing acute brain dysfunction (ABD), including delirium and coma in the intensive care unit (ICU), is a critical challenge due to its prevalence and severe implications for patient outcomes. Current diagnostic methods rely on infrequent clinical observations, which can only determine a patient's ABD status after onset. Our research attempts to solve these problems by harnessing Electronic Health Records (EHR) data to develop automated methods for ABD prediction for patients in the ICU. Existing models solely predict a single state (e.g., either delirium or coma), require at least 24 hours of observation data to make predictions, do not dynamically predict fluctuating ABD conditions during ICU stay (typically a one-time prediction), and use small sample size, proprietary single-hospital datasets. Our research fills these gaps in the existing literature by dynamically predicting delirium, coma, and mortality for 12-hour intervals throughout an ICU stay and validating on two public datasets. Our research also introduces the concept of dynamically predicting critical transitions from non-ABD to ABD and between different ABD states in real time, which could be clinically more informative for the hospital staff. We compared the predictive performance of two state-of-the-art neural network models, the MAMBA selective state space model and the Longformer Transformer model. Using the MAMBA model, we achieved a mean area under the receiving operator characteristic curve (AUROC) of 0.95 on outcome prediction of ABD for 12-hour intervals. The model achieves a mean AUROC of 0.79 when predicting transitions between ABD states. Our study uses a curated dataset from the University of Florida Health Shands Hospital for internal validation and two publicly available datasets, MIMIC-IV and eICU, for external validation, demonstrating robustness across ICU stays from 203 hospitals and 140,945 patients.
Leveraging Computer Vision in the Intensive Care Unit (ICU) for Examining Visitation and Mobility
Mar 10, 2024



Despite the importance of closely monitoring patients in the Intensive Care Unit (ICU), many aspects are still assessed in a limited manner due to the time constraints imposed on healthcare providers. For example, although excessive visitations during rest hours can potentially exacerbate the risk of circadian rhythm disruption and delirium, it is not captured in the ICU. Likewise, while mobility can be an important indicator of recovery or deterioration in ICU patients, it is only captured sporadically or not captured at all. In the past few years, the computer vision field has found application in many domains by reducing the human burden. Using computer vision systems in the ICU can also potentially enable non-existing assessments or enhance the frequency and accuracy of existing assessments while reducing the staff workload. In this study, we leverage a state-of-the-art noninvasive computer vision system based on depth imaging to characterize ICU visitations and patients' mobility. We then examine the relationship between visitation and several patient outcomes, such as pain, acuity, and delirium. We found an association between deteriorating patient acuity and the incidence of delirium with increased visitations. In contrast, self-reported pain, reported using the Defense and Veteran Pain Rating Scale (DVPRS), was correlated with decreased visitations. Our findings highlight the feasibility and potential of using noninvasive autonomous systems to monitor ICU patients.
APRICOT: Acuity Prediction in Intensive Care Unit (ICU): Predicting Stability, Transitions, and Life-Sustaining Therapies
Nov 03, 2023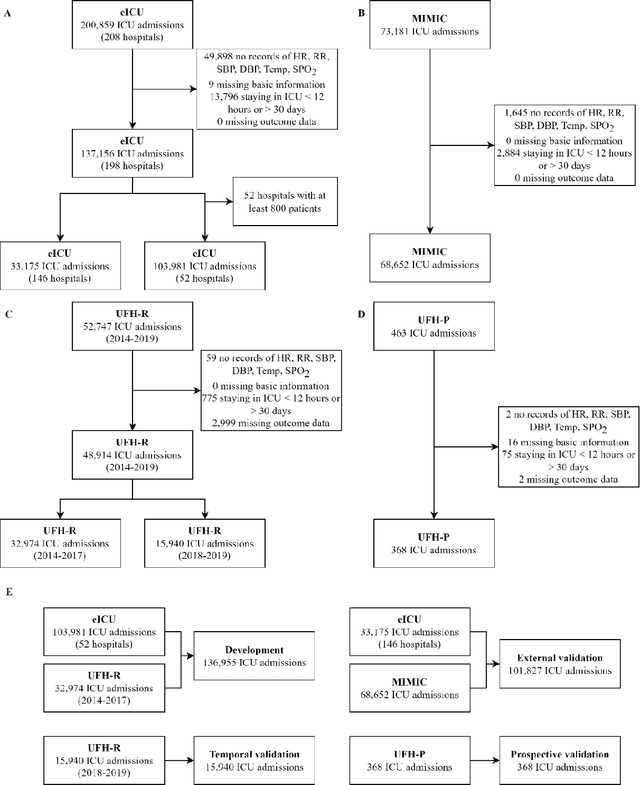

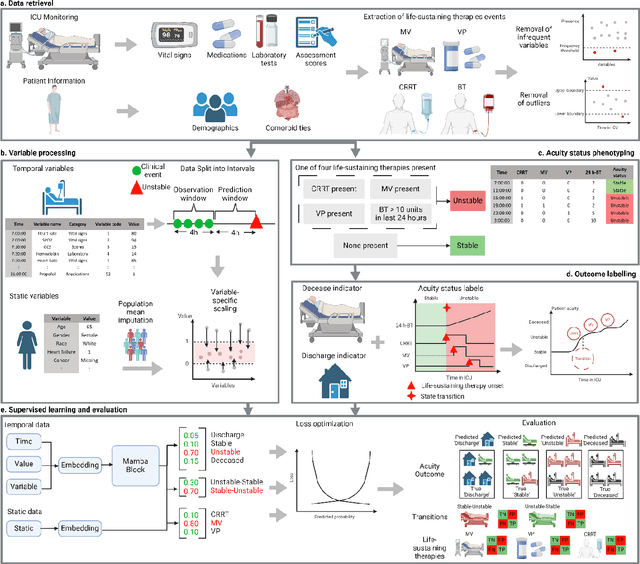
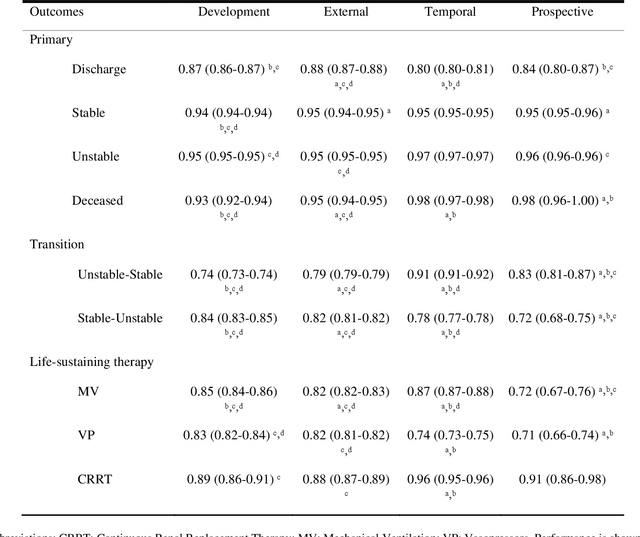
The acuity state of patients in the intensive care unit (ICU) can quickly change from stable to unstable, sometimes leading to life-threatening conditions. Early detection of deteriorating conditions can result in providing more timely interventions and improved survival rates. Current approaches rely on manual daily assessments. Some data-driven approaches have been developed, that use mortality as a proxy of acuity in the ICU. However, these methods do not integrate acuity states to determine the stability of a patient or the need for life-sustaining therapies. In this study, we propose APRICOT (Acuity Prediction in Intensive Care Unit), a Transformer-based neural network to predict acuity state in real-time in ICU patients. We develop and extensively validate externally, temporally, and prospectively the APRICOT model on three large datasets: University of Florida Health (UFH), eICU Collaborative Research Database (eICU), and Medical Information Mart for Intensive Care (MIMIC)-IV. The performance of APRICOT shows comparable results to state-of-the-art mortality prediction models (external AUROC 0.93-0.93, temporal AUROC 0.96-0.98, and prospective AUROC 0.98) as well as acuity prediction models (external AUROC 0.80-0.81, temporal AUROC 0.77-0.78, and prospective AUROC 0.87). Furthermore, APRICOT can make predictions for the need for life-sustaining therapies, showing comparable results to state-of-the-art ventilation prediction models (external AUROC 0.80-0.81, temporal AUROC 0.87-0.88, and prospective AUROC 0.85), and vasopressor prediction models (external AUROC 0.82-0.83, temporal AUROC 0.73-0.75, prospective AUROC 0.87). This tool allows for real-time acuity monitoring of a patient and can provide helpful information to clinicians to make timely interventions. Furthermore, the model can suggest life-sustaining therapies that the patient might need in the next hours in the ICU.
Transformers in Healthcare: A Survey
Jun 30, 2023



With Artificial Intelligence (AI) increasingly permeating various aspects of society, including healthcare, the adoption of the Transformers neural network architecture is rapidly changing many applications. Transformer is a type of deep learning architecture initially developed to solve general-purpose Natural Language Processing (NLP) tasks and has subsequently been adapted in many fields, including healthcare. In this survey paper, we provide an overview of how this architecture has been adopted to analyze various forms of data, including medical imaging, structured and unstructured Electronic Health Records (EHR), social media, physiological signals, and biomolecular sequences. Those models could help in clinical diagnosis, report generation, data reconstruction, and drug/protein synthesis. We identified relevant studies using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. We also discuss the benefits and limitations of using transformers in healthcare and examine issues such as computational cost, model interpretability, fairness, alignment with human values, ethical implications, and environmental impact.
Transformer Models for Acute Brain Dysfunction Prediction
Mar 13, 2023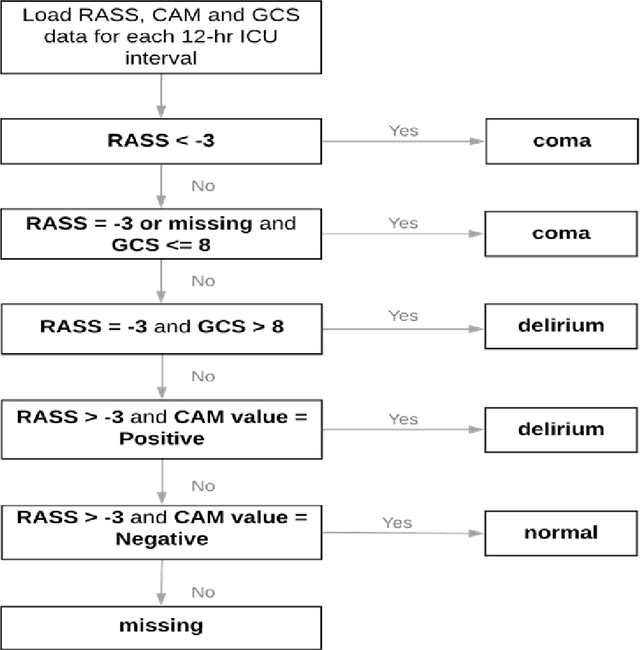

Acute brain dysfunctions (ABD), which include coma and delirium, are prevalent in the ICU, especially among older patients. The current approach in manual assessment of ABD by care providers may be sporadic and subjective. Hence, there exists a need for a data-driven robust system automating the assessment and prediction of ABD. In this work, we develop a machine learning system for real-time prediction of ADB using Electronic Health Record (HER) data. Our data processing pipeline enables integration of static and temporal data, and extraction of features relevant to ABD. We train several state-of-the-art transformer models and baseline machine learning models including CatBoost and XGB on the data that was collected from patients admitted to the ICU at UF Shands Hospital. We demonstrate the efficacy of our system for tasks related to acute brain dysfunction including binary classification of brain acuity and multi-class classification (i.e., coma, delirium, death, or normal), achieving a mean AUROC of 0.953 on our Long-former implementation. Our system can then be deployed for real-time prediction of ADB in ICUs to reduce the number of incidents caused by ABD. Moreover, the real-time system has the potential to reduce costs, duration of patients stays in the ICU, and mortality among those afflicted.