 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeUncertainty-Aware Shape Estimation of a Surgical Continuum Manipulator in Constrained Environments using Fiber Bragg Grating Sensors
May 11, 2024



Continuum Dexterous Manipulators (CDMs) are well-suited tools for minimally invasive surgery due to their inherent dexterity and reachability. Nonetheless, their flexible structure and non-linear curvature pose significant challenges for shape-based feedback control. The use of Fiber Bragg Grating (FBG) sensors for shape sensing has shown great potential in estimating the CDM's tip position and subsequently reconstructing the shape using optimization algorithms. This optimization, however, is under-constrained and may be ill-posed for complex shapes, falling into local minima. In this work, we introduce a novel method capable of directly estimating a CDM's shape from FBG sensor wavelengths using a deep neural network. In addition, we propose the integration of uncertainty estimation to address the critical issue of uncertainty in neural network predictions. Neural network predictions are unreliable when the input sample is outside the training distribution or corrupted by noise. Recognizing such deviations is crucial when integrating neural networks within surgical robotics, as inaccurate estimations can pose serious risks to the patient. We present a robust method that not only improves the precision upon existing techniques for FBG-based shape estimation but also incorporates a mechanism to quantify the models' confidence through uncertainty estimation. We validate the uncertainty estimation through extensive experiments, demonstrating its effectiveness and reliability on out-of-distribution (OOD) data, adding an additional layer of safety and precision to minimally invasive surgical robotics.
SyntheX: Scaling Up Learning-based X-ray Image Analysis Through In Silico Experiments
Jun 13, 2022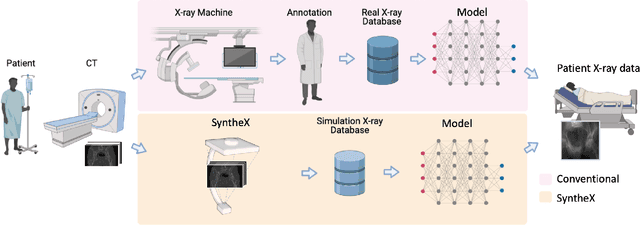
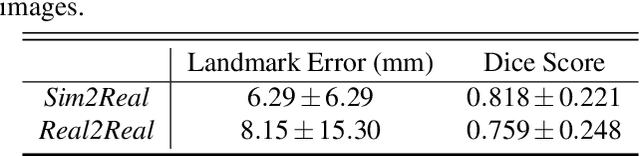
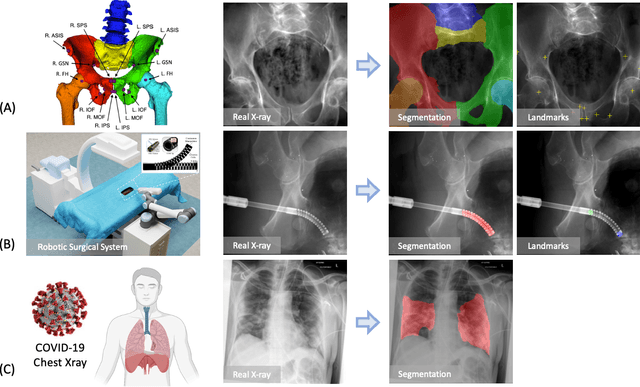
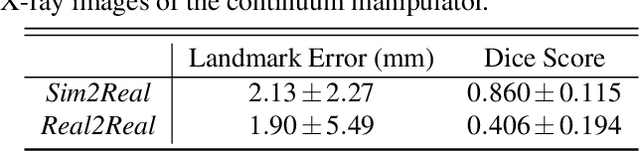
Artificial intelligence (AI) now enables automated interpretation of medical images for clinical use. However, AI's potential use for interventional images (versus those involved in triage or diagnosis), such as for guidance during surgery, remains largely untapped. This is because surgical AI systems are currently trained using post hoc analysis of data collected during live surgeries, which has fundamental and practical limitations, including ethical considerations, expense, scalability, data integrity, and a lack of ground truth. Here, we demonstrate that creating realistic simulated images from human models is a viable alternative and complement to large-scale in situ data collection. We show that training AI image analysis models on realistically synthesized data, combined with contemporary domain generalization or adaptation techniques, results in models that on real data perform comparably to models trained on a precisely matched real data training set. Because synthetic generation of training data from human-based models scales easily, we find that our model transfer paradigm for X-ray image analysis, which we refer to as SyntheX, can even outperform real data-trained models due to the effectiveness of training on a larger dataset. We demonstrate the potential of SyntheX on three clinical tasks: Hip image analysis, surgical robotic tool detection, and COVID-19 lung lesion segmentation. SyntheX provides an opportunity to drastically accelerate the conception, design, and evaluation of intelligent systems for X-ray-based medicine. In addition, simulated image environments provide the opportunity to test novel instrumentation, design complementary surgical approaches, and envision novel techniques that improve outcomes, save time, or mitigate human error, freed from the ethical and practical considerations of live human data collection.
Pose Estimation of Periacetabular Osteotomy Fragments with Intraoperative X-Ray Navigation
Mar 22, 2019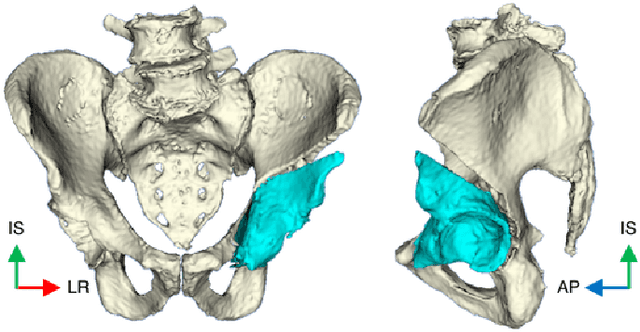
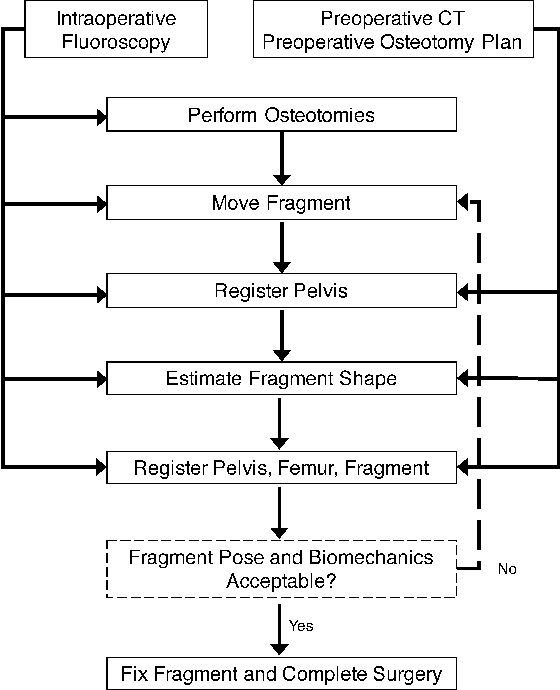

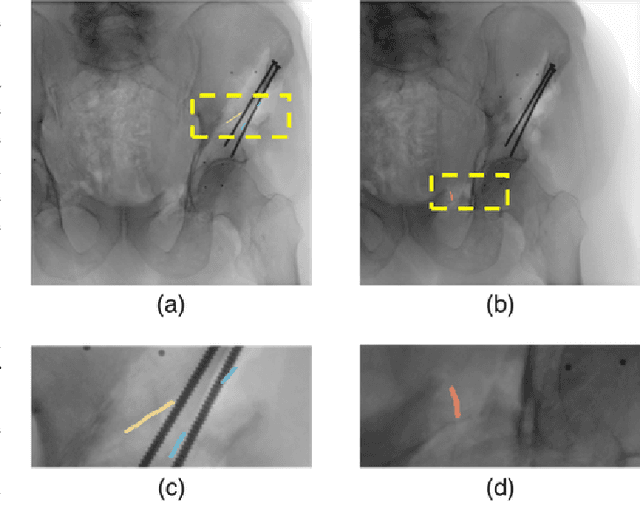
Objective: State of the art navigation systems for pelvic osteotomies use optical systems with external fiducials. We propose the use of X-Ray navigation for pose estimation of periacetabular fragments without fiducials. Methods: A 2D/3D registration pipeline was developed to recover fragment pose. This pipeline was tested through an extensive simulation study and 6 cadaveric surgeries. Using osteotomy boundaries in the fluoroscopic images, the preoperative plan is refined to more accurately match the intraoperative shape. Results: In simulation, average fragment pose errors were 1.3{\deg}/1.7 mm when the planned fragment matched the intraoperative fragment, 2.2{\deg}/2.1 mm when the plan was not updated to match the true shape, and 1.9{\deg}/2.0 mm when the fragment shape was intraoperatively estimated. In cadaver experiments, the average pose errors were 2.2{\deg}/2.2 mm, 3.8{\deg}/2.5 mm, and 3.5{\deg}/2.2 mm when registering with the actual fragment shape, a preoperative plan, and an intraoperatively refined plan, respectively. Average errors of the lateral center edge angle were less than 2{\deg} for all fragment shapes in simulation and cadaver experiments. Conclusion: The proposed pipeline is capable of accurately reporting femoral head coverage within a range clinically identified for long-term joint survivability. Significance: Human interpretation of fragment pose is challenging and usually restricted to rotation about a single anatomical axis. The proposed pipeline provides an intraoperative estimate of rigid pose with respect to all anatomical axes, is compatible with minimally invasive incisions, and has no dependence on external fiducials.