 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeFrom Monocular Vision to Autonomous Action: Guiding Tumor Resection via 3D Reconstruction
Mar 20, 2025Surgical automation requires precise guidance and understanding of the scene. Current methods in the literature rely on bulky depth cameras to create maps of the anatomy, however this does not translate well to space-limited clinical applications. Monocular cameras are small and allow minimally invasive surgeries in tight spaces but additional processing is required to generate 3D scene understanding. We propose a 3D mapping pipeline that uses only RGB images to create segmented point clouds of the target anatomy. To ensure the most precise reconstruction, we compare different structure from motion algorithms' performance on mapping the central airway obstructions, and test the pipeline on a downstream task of tumor resection. In several metrics, including post-procedure tissue model evaluation, our pipeline performs comparably to RGB-D cameras and, in some cases, even surpasses their performance. These promising results demonstrate that automation guidance can be achieved in minimally invasive procedures with monocular cameras. This study is a step toward the complete autonomy of surgical robots.
Estimation of Trocar and Tool Interaction Forces on the da Vinci Research Kit with Two-Step Deep Learning
Dec 11, 2020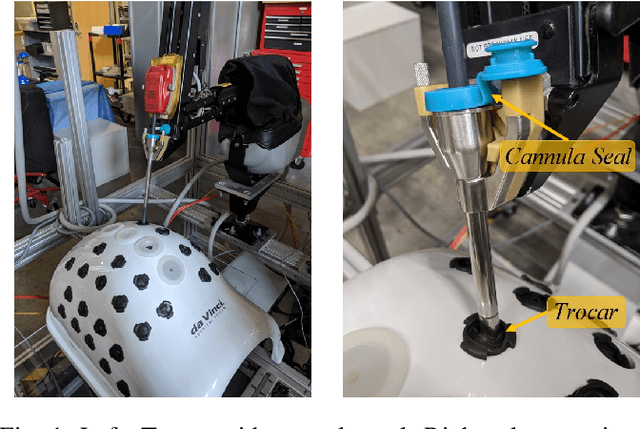

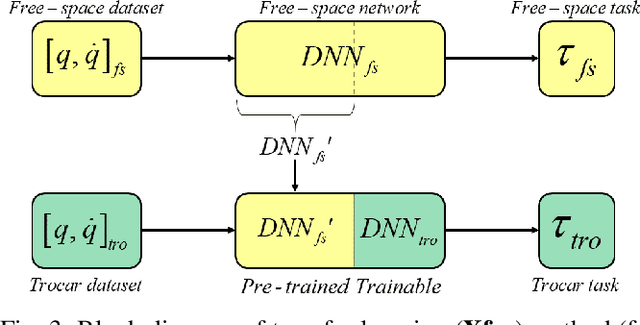
Measurement of environment interaction forces during robotic minimally-invasive surgery would enable haptic feedback to the surgeon, thereby solving one long-standing limitation. Estimating this force from existing sensor data avoids the challenge of retrofitting systems with force sensors, but is difficult due to mechanical effects such as friction and compliance in the robot mechanism. We have previously shown that neural networks can be trained to estimate the internal robot joint torques, thereby enabling estimation of external forces. In this work, we extend the method to estimate external Cartesian forces and torques, and also present a two-step approach to adapt to the specific surgical setup by compensating for forces due to the interactions between the instrument shaft and cannula seal and between the trocar and patient body. Experiments show that this approach provides estimates of external forces and torques within a mean root-mean-square error (RMSE) of 2 N and 0.08 Nm, respectively. Furthermore, the two-step approach can add as little as 5 minutes to the surgery setup time, with about 4 minutes to collect intraoperative training data and 1 minute to train the second-step network.