 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeMitigating Degree Bias Adaptively with Hard-to-Learn Nodes in Graph Contrastive Learning
Jun 05, 2025Graph Neural Networks (GNNs) often suffer from degree bias in node classification tasks, where prediction performance varies across nodes with different degrees. Several approaches, which adopt Graph Contrastive Learning (GCL), have been proposed to mitigate this bias. However, the limited number of positive pairs and the equal weighting of all positives and negatives in GCL still lead to low-degree nodes acquiring insufficient and noisy information. This paper proposes the Hardness Adaptive Reweighted (HAR) contrastive loss to mitigate degree bias. It adds more positive pairs by leveraging node labels and adaptively weights positive and negative pairs based on their learning hardness. In addition, we develop an experimental framework named SHARP to extend HAR to a broader range of scenarios. Both our theoretical analysis and experiments validate the effectiveness of SHARP. The experimental results across four datasets show that SHARP achieves better performance against baselines at both global and degree levels.
ProxiMix: Enhancing Fairness with Proximity Samples in Subgroups
Oct 02, 2024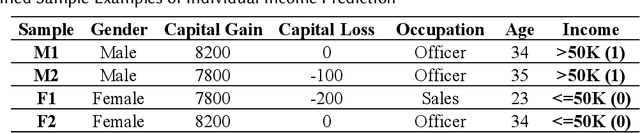
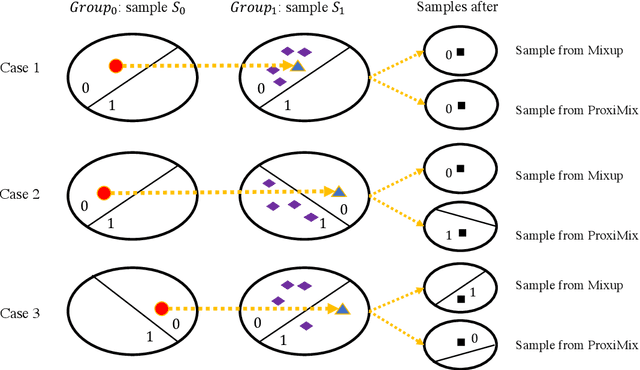
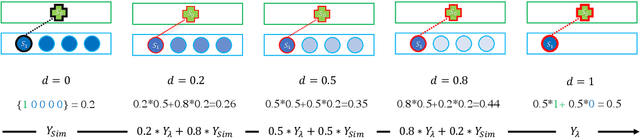

Many bias mitigation methods have been developed for addressing fairness issues in machine learning. We found that using linear mixup alone, a data augmentation technique, for bias mitigation, can still retain biases present in dataset labels. Research presented in this paper aims to address this issue by proposing a novel pre-processing strategy in which both an existing mixup method and our new bias mitigation algorithm can be utilized to improve the generation of labels of augmented samples, which are proximity aware. Specifically, we proposed ProxiMix which keeps both pairwise and proximity relationships for fairer data augmentation. We conducted thorough experiments with three datasets, three ML models, and different hyperparameters settings. Our experimental results showed the effectiveness of ProxiMix from both fairness of predictions and fairness of recourse perspectives.
Progressively refined deep joint registration segmentation (ProRSeg) of gastrointestinal organs at risk: Application to MRI and cone-beam CT
Oct 25, 2022



Method: ProRSeg was trained using 5-fold cross-validation with 110 T2-weighted MRI acquired at 5 treatment fractions from 10 different patients, taking care that same patient scans were not placed in training and testing folds. Segmentation accuracy was measured using Dice similarity coefficient (DSC) and Hausdorff distance at 95th percentile (HD95). Registration consistency was measured using coefficient of variation (CV) in displacement of OARs. Ablation tests and accuracy comparisons against multiple methods were done. Finally, applicability of ProRSeg to segment cone-beam CT (CBCT) scans was evaluated on 80 scans using 5-fold cross-validation. Results: ProRSeg processed 3D volumes (128 $\times$ 192 $\times$ 128) in 3 secs on a NVIDIA Tesla V100 GPU. It's segmentations were significantly more accurate ($p<0.001$) than compared methods, achieving a DSC of 0.94 $\pm$0.02 for liver, 0.88$\pm$0.04 for large bowel, 0.78$\pm$0.03 for small bowel and 0.82$\pm$0.04 for stomach-duodenum from MRI. ProRSeg achieved a DSC of 0.72$\pm$0.01 for small bowel and 0.76$\pm$0.03 for stomach-duodenum from CBCT. ProRSeg registrations resulted in the lowest CV in displacement (stomach-duodenum $CV_{x}$: 0.75\%, $CV_{y}$: 0.73\%, and $CV_{z}$: 0.81\%; small bowel $CV_{x}$: 0.80\%, $CV_{y}$: 0.80\%, and $CV_{z}$: 0.68\%; large bowel $CV_{x}$: 0.71\%, $CV_{y}$ : 0.81\%, and $CV_{z}$: 0.75\%). ProRSeg based dose accumulation accounting for intra-fraction (pre-treatment to post-treatment MRI scan) and inter-fraction motion showed that the organ dose constraints were violated in 4 patients for stomach-duodenum and for 3 patients for small bowel. Study limitations include lack of independent testing and ground truth phantom datasets to measure dose accumulation accuracy.