 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeMonocular Marker-free Patient-to-Image Intraoperative Registration for Cochlear Implant Surgery
May 23, 2025This paper presents a novel method for monocular patient-to-image intraoperative registration, specifically designed to operate without any external hardware tracking equipment or fiducial point markers. Leveraging a synthetic microscopy surgical scene dataset with a wide range of transformations, our approach directly maps preoperative CT scans to 2D intraoperative surgical frames through a lightweight neural network for real-time cochlear implant surgery guidance via a zero-shot learning approach. Unlike traditional methods, our framework seamlessly integrates with monocular surgical microscopes, making it highly practical for clinical use without additional hardware dependencies and requirements. Our method estimates camera poses, which include a rotation matrix and a translation vector, by learning from the synthetic dataset, enabling accurate and efficient intraoperative registration. The proposed framework was evaluated on nine clinical cases using a patient-specific and cross-patient validation strategy. Our results suggest that our approach achieves clinically relevant accuracy in predicting 6D camera poses for registering 3D preoperative CT scans to 2D surgical scenes with an angular error within 10 degrees in most cases, while also addressing limitations of traditional methods, such as reliance on external tracking systems or fiducial markers.
Weakly-supervised Mamba-Based Mastoidectomy Shape Prediction for Cochlear Implant Surgery Using 3D T-Distribution Loss
May 23, 2025Cochlear implant surgery is a treatment for individuals with severe hearing loss. It involves inserting an array of electrodes inside the cochlea to electrically stimulate the auditory nerve and restore hearing sensation. A crucial step in this procedure is mastoidectomy, a surgical intervention that removes part of the mastoid region of the temporal bone, providing a critical pathway to the cochlea for electrode placement. Accurate prediction of the mastoidectomy region from preoperative imaging assists presurgical planning, reduces surgical risks, and improves surgical outcomes. In previous work, a self-supervised network was introduced to predict the mastoidectomy region using only preoperative CT scans. While promising, the method suffered from suboptimal robustness, limiting its practical application. To address this limitation, we propose a novel weakly-supervised Mamba-based framework to predict accurate mastoidectomy regions directly from preoperative CT scans. Our approach utilizes a 3D T-Distribution loss function inspired by the Student-t distribution, which effectively handles the complex geometric variability inherent in mastoidectomy shapes. Weak supervision is achieved using the segmentation results from the prior self-supervised network to eliminate the need for manual data cleaning or labeling throughout the training process. The proposed method is extensively evaluated against state-of-the-art approaches, demonstrating superior performance in predicting accurate and clinically relevant mastoidectomy regions. Our findings highlight the robustness and efficiency of the weakly-supervised learning framework with the proposed novel 3D T-Distribution loss.
Cochlear Implantation of Slim Pre-curved Arrays using Automatic Pre-operative Insertion Plans
Oct 24, 2024Hypothesis: Pre-operative cochlear implant (CI) electrode array (EL) insertion plans created by automated image analysis methods can improve positioning of slim pre-curved EL. Background: This study represents the first evaluation of a system for patient-customized EL insertion planning for a slim pre-curved EL. Methods: Twenty-one temporal bone specimens were divided into experimental and control groups and underwent cochlear implantation. For the control group, the surgeon performed a traditional insertion without an insertion plan. For the experimental group, customized insertion plans guided entry site, trajectory, curl direction, and base insertion depth. An additional 35 clinical insertions from the same surgeon were analyzed, 7 of which were conducted using the insertion plans. EL positioning was analyzed using post-operative imaging auto-segmentation techniques, allowing measurement of angular insertion depth (AID), mean modiolar distance (MMD), and scalar position. Results: In the cadaveric temporal bones, 3 scalar translocations, including 2 foldovers, occurred in 14 control group insertions. In the clinical insertions, translocations occurred in 2 of 28 control cases. No translocations or folds occurred in the 7 experimental temporal bone and the 7 experimental clinical insertions. Among the non-translocated cases, overall AID and MMD were 401(41) degrees and 0.34(0.13) mm for the control insertions. AID and MMD for the experimental insertions were 424(43) degrees and 0.34(0.09) mm overall and were 432(19) and 0.30(0.07) mm for cases where the planned insertion depth was achieved. Conclusions: Trends toward improved EL positioning within scala tympani were observed when EL insertion plans are used. Variability in MMD was significantly reduced (0.07mm vs 0.13 mm, p=0.039) when the planned depth was achieved.
Unsupervised Mastoidectomy for Cochlear CT Mesh Reconstruction Using Highly Noisy Data
Jul 22, 2024Cochlear Implant (CI) procedures involve inserting an array of electrodes into the cochlea located inside the inner ear. Mastoidectomy is a surgical procedure that uses a high-speed drill to remove part of the mastoid region of the temporal bone, providing safe access to the cochlea through the middle and inner ear. We aim to develop an intraoperative navigation system that registers plans created using 3D preoperative Computerized Tomography (CT) volumes with the 2D surgical microscope view. Herein, we propose a method to synthesize the mastoidectomy volume using only the preoperative CT scan, where the mastoid is intact. We introduce an unsupervised learning framework designed to synthesize mastoidectomy. For model training purposes, this method uses postoperative CT scans to avoid manual data cleaning or labeling, even when the region removed during mastoidectomy is visible but affected by metal artifacts, low signal-to-noise ratio, or electrode wiring. Our approach estimates mastoidectomy regions with a mean dice score of 70.0%. This approach represents a major step forward for CI intraoperative navigation by predicting realistic mastoidectomy-removed regions in preoperative planning that can be used to register the pre-surgery plan to intraoperative microscopy.
Monocular Microscope to CT Registration using Pose Estimation of the Incus for Augmented Reality Cochlear Implant Surgery
Mar 12, 2024For those experiencing severe-to-profound sensorineural hearing loss, the cochlear implant (CI) is the preferred treatment. Augmented reality (AR) aided surgery can potentially improve CI procedures and hearing outcomes. Typically, AR solutions for image-guided surgery rely on optical tracking systems to register pre-operative planning information to the display so that hidden anatomy or other important information can be overlayed and co-registered with the view of the surgical scene. In this paper, our goal is to develop a method that permits direct 2D-to-3D registration of the microscope video to the pre-operative Computed Tomography (CT) scan without the need for external tracking equipment. Our proposed solution involves using surface mapping of a portion of the incus in surgical recordings and determining the pose of this structure relative to the surgical microscope by performing pose estimation via the perspective-n-point (PnP) algorithm. This registration can then be applied to pre-operative segmentations of other anatomy-of-interest, as well as the planned electrode insertion trajectory to co-register this information for the AR display. Our results demonstrate the accuracy with an average rotation error of less than 25 degrees and a translation error of less than 2 mm, 3 mm, and 0.55% for the x, y, and z axes, respectively. Our proposed method has the potential to be applicable and generalized to other surgical procedures while only needing a monocular microscope during intra-operation.
DABS-LS: Deep Atlas-Based Segmentation Using Regional Level Set Self-Supervision
Feb 16, 2024Cochlear implants (CIs) are neural prosthetics used to treat patients with severe-to-profound hearing loss. Patient-specific modeling of CI stimulation of the auditory nerve fiber (ANFs) can help audiologists improve the CI programming. These models require localization of the ANFs relative to surrounding anatomy and the CI. Localization is challenging because the ANFs are so small they are not directly visible in clinical imaging. In this work, we hypothesize the position of the ANFs can be accurately inferred from the location of the internal auditory canal (IAC), which has high contrast in CT, since the ANFs pass through this canal between the cochlea and the brain. Inspired by VoxelMorph, in this paper we propose a deep atlas-based IAC segmentation network. We create a single atlas in which the IAC and ANFs are pre-localized. Our network is trained to produce deformation fields (DFs) mapping coordinates from the atlas to new target volumes and that accurately segment the IAC. We hypothesize that DFs that accurately segment the IAC in target images will also facilitate accurate atlas-based localization of the ANFs. As opposed to VoxelMorph, which aims to produce DFs that accurately register the entire volume, our novel contribution is an entirely self-supervised training scheme that aims to produce DFs that accurately segment the target structure. This self-supervision is facilitated using a regional level set (LS) inspired loss function. We call our method Deep Atlas Based Segmentation using Level Sets (DABS-LS). Results show that DABS-LS outperforms VoxelMorph for IAC segmentation. Tests with publicly available datasets for trachea and kidney segmentation also show significant improvement in segmentation accuracy, demonstrating the generalizability of the method.
Atlas-Based Segmentation of Intracochlear Anatomy in Metal Artifact Affected CT Images of the Ear with Co-trained Deep Neural Networks
Jul 09, 2021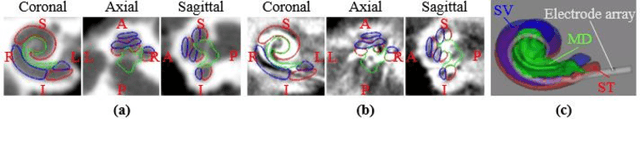
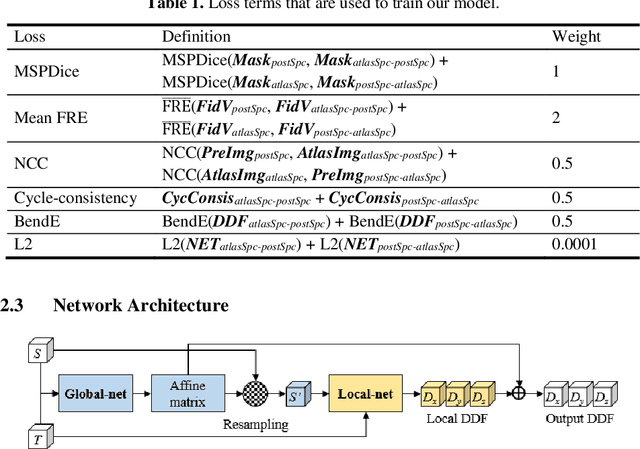
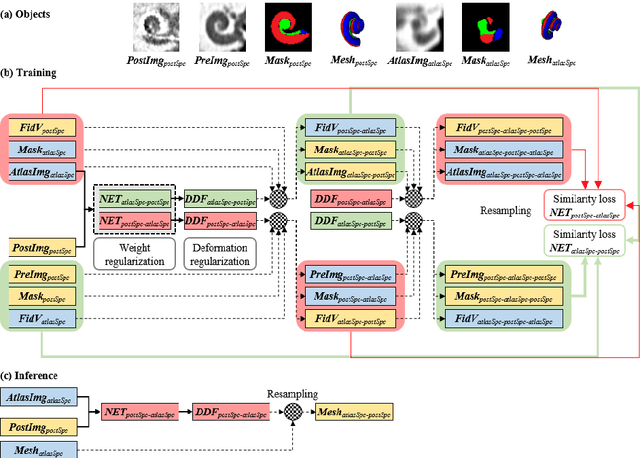
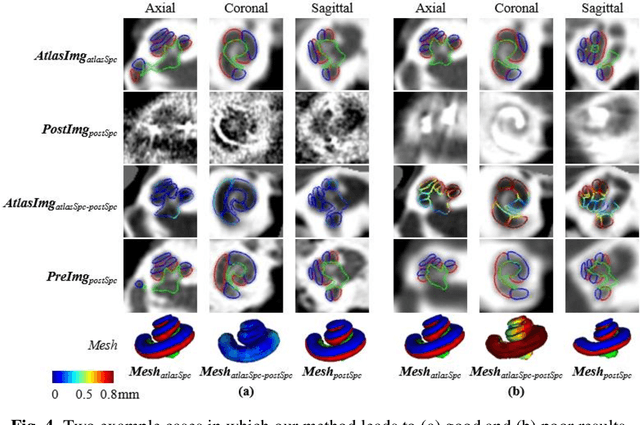
We propose an atlas-based method to segment the intracochlear anatomy (ICA) in the post-implantation CT (Post-CT) images of cochlear implant (CI) recipients that preserves the point-to-point correspondence between the meshes in the atlas and the segmented volumes. To solve this problem, which is challenging because of the strong artifacts produced by the implant, we use a pair of co-trained deep networks that generate dense deformation fields (DDFs) in opposite directions. One network is tasked with registering an atlas image to the Post-CT images and the other network is tasked with registering the Post-CT images to the atlas image. The networks are trained using loss functions based on voxel-wise labels, image content, fiducial registration error, and cycle-consistency constraint. The segmentation of the ICA in the Post-CT images is subsequently obtained by transferring the predefined segmentation meshes of the ICA in the atlas image to the Post-CT images using the corresponding DDFs generated by the trained registration networks. Our model can learn the underlying geometric features of the ICA even though they are obscured by the metal artifacts. We show that our end-to-end network produces results that are comparable to the current state of the art (SOTA) that relies on a two-steps approach that first uses conditional generative adversarial networks to synthesize artifact-free images from the Post-CT images and then uses an active shape model-based method to segment the ICA in the synthetic images. Our method requires a fraction of the time needed by the SOTA, which is important for end-user acceptance.
Validation of image-guided cochlear implant programming techniques
Sep 23, 2019

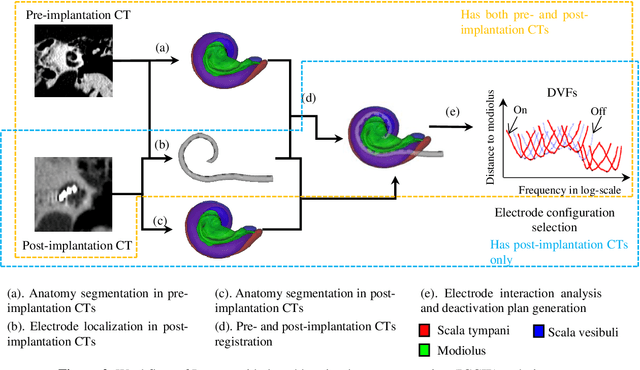

Cochlear implants (CIs) are a standard treatment for patients who experience severe to profound hearing loss. Recent studies have shown that hearing outcome is correlated with intra-cochlear anatomy and electrode placement. Our group has developed image-guided CI programming (IGCIP) techniques that use image analysis methods to both segment the inner ear structures in pre- or post-implantation CT images and localize the CI electrodes in post-implantation CT images. This permits to assist audiologists with CI programming by suggesting which among the contacts should be deactivated to reduce electrode interaction that is known to affect outcomes. Clinical studies have shown that IGCIP can improve hearing outcomes for CI recipients. However, the sensitivity of IGCIP with respect to the accuracy of the two major steps: electrode localization and intra-cochlear anatomy segmentation, is unknown. In this article, we create a ground truth dataset with conventional CT and micro-CT images of 35 temporal bone specimens to both rigorously characterize the accuracy of these two steps and assess how inaccuracies in these steps affect the overall results. Our study results show that when clinical pre- and post-implantation CTs are available, IGCIP produces results that are comparable to those obtained with the corresponding ground truth in 86.7% of the subjects tested. When only post-implantation CTs are available, this number is 83.3%. These results suggest that our current method is robust to errors in segmentation and localization but also that it can be improved upon. Keywords: cochlear implant, ground truth, segmentation, validation
Accurate Detection of Inner Ears in Head CTs Using a Deep Volume-to-Volume Regression Network with False Positive Suppression and a Shape-Based Constraint
Jun 12, 2018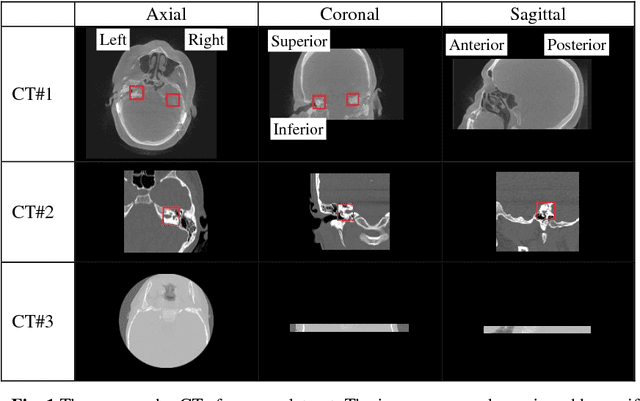
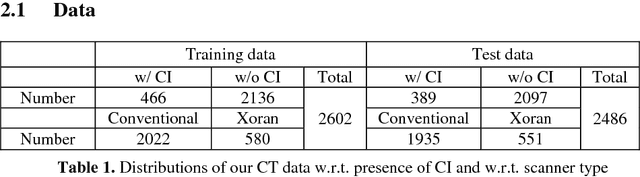
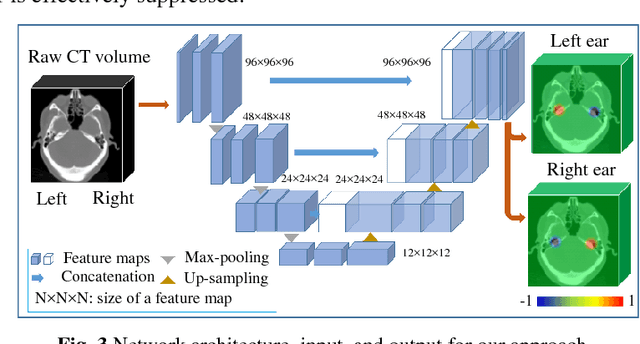
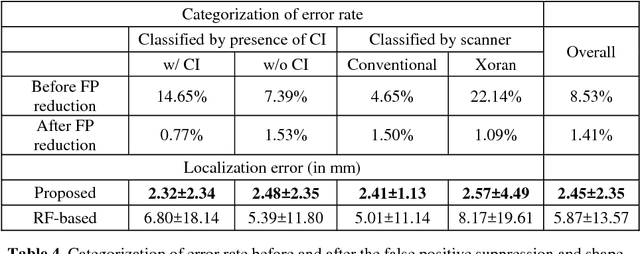
Cochlear implants (CIs) are neural prosthetics which are used to treat patients with hearing loss. CIs use an array of electrodes which are surgically inserted into the cochlea to stimulate the auditory nerve endings. After surgery, CIs need to be programmed. Studies have shown that the spatial relationship between the intra-cochlear anatomy and electrodes derived from medical images can guide CI programming and lead to significant improvement in hearing outcomes. However, clinical head CT images are usually obtained from scanners of different brands with different protocols. The field of view thus varies greatly and visual inspection is needed to document their content prior to applying algorithms for electrode localization and intra-cochlear anatomy segmentation. In this work, to determine the presence/absence of inner ears and to accurately localize them in head CTs, we use a volume-to-volume convolutional neural network which can be trained end-to-end to map a raw CT volume to probability maps which indicate inner ear positions. We incorporate a false positive suppression strategy in training and apply a shape-based constraint. We achieve a labeling accuracy of 98.59% and a localization error of 2.45mm. The localization error is significantly smaller than a random forest-based approach that has been proposed recently to perform the same task.