 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeTowards Reducing Diagnostic Errors with Interpretable Risk Prediction
Feb 15, 2024Many diagnostic errors occur because clinicians cannot easily access relevant information in patient Electronic Health Records (EHRs). In this work we propose a method to use LLMs to identify pieces of evidence in patient EHR data that indicate increased or decreased risk of specific diagnoses; our ultimate aim is to increase access to evidence and reduce diagnostic errors. In particular, we propose a Neural Additive Model to make predictions backed by evidence with individualized risk estimates at time-points where clinicians are still uncertain, aiming to specifically mitigate delays in diagnosis and errors stemming from an incomplete differential. To train such a model, it is necessary to infer temporally fine-grained retrospective labels of eventual "true" diagnoses. We do so with LLMs, to ensure that the input text is from before a confident diagnosis can be made. We use an LLM to retrieve an initial pool of evidence, but then refine this set of evidence according to correlations learned by the model. We conduct an in-depth evaluation of the usefulness of our approach by simulating how it might be used by a clinician to decide between a pre-defined list of differential diagnoses.
Retrieving Evidence from EHRs with LLMs: Possibilities and Challenges
Sep 08, 2023



Unstructured Electronic Health Record (EHR) data often contains critical information complementary to imaging data that would inform radiologists' diagnoses. However, time constraints and the large volume of notes frequently associated with individual patients renders manual perusal of such data to identify relevant evidence infeasible in practice. Modern Large Language Models (LLMs) provide a flexible means of interacting with unstructured EHR data, and may provide a mechanism to efficiently retrieve and summarize unstructured evidence relevant to a given query. In this work, we propose and evaluate an LLM (Flan-T5 XXL) for this purpose. Specifically, in a zero-shot setting we task the LLM to infer whether a patient has or is at risk of a particular condition; if so, we prompt the model to summarize the supporting evidence. Enlisting radiologists for manual evaluation, we find that this LLM-based approach provides outputs consistently preferred to a standard information retrieval baseline, but we also highlight the key outstanding challenge: LLMs are prone to hallucinating evidence. However, we provide results indicating that model confidence in outputs might indicate when LLMs are hallucinating, potentially providing a means to address this.
CHiLL: Zero-shot Custom Interpretable Feature Extraction from Clinical Notes with Large Language Models
Feb 23, 2023



Large Language Models (LLMs) have yielded fast and dramatic progress in NLP, and now offer strong few- and zero-shot capabilities on new tasks, reducing the need for annotation. This is especially exciting for the medical domain, in which supervision is often scant and expensive. At the same time, model predictions are rarely so accurate that they can be trusted blindly. Clinicians therefore tend to favor "interpretable" classifiers over opaque LLMs. For example, risk prediction tools are often linear models defined over manually crafted predictors that must be laboriously extracted from EHRs. We propose CHiLL (Crafting High-Level Latents), which uses LLMs to permit natural language specification of high-level features for linear models via zero-shot feature extraction using expert-composed queries. This approach has the promise to empower physicians to use their domain expertise to craft features which are clinically meaningful for a downstream task of interest, without having to manually extract these from raw EHR (as often done now). We are motivated by a real-world risk prediction task, but as a reproducible proxy, we use MIMIC-III and MIMIC-CXR data and standard predictive tasks (e.g., 30-day readmission) to evaluate our approach. We find that linear models using automatically extracted features are comparably performant to models using reference features, and provide greater interpretability than linear models using "Bag-of-Words" features. We verify that learned feature weights align well with clinical expectations.
That's the Wrong Lung! Evaluating and Improving the Interpretability of Unsupervised Multimodal Encoders for Medical Data
Oct 12, 2022



Pretraining multimodal models on Electronic Health Records (EHRs) provides a means of learning representations that can transfer to downstream tasks with minimal supervision. Recent multimodal models induce soft local alignments between image regions and sentences. This is of particular interest in the medical domain, where alignments might highlight regions in an image relevant to specific phenomena described in free-text. While past work has suggested that attention "heatmaps" can be interpreted in this manner, there has been little evaluation of such alignments. We compare alignments from a state-of-the-art multimodal (image and text) model for EHR with human annotations that link image regions to sentences. Our main finding is that the text has an often weak or unintuitive influence on attention; alignments do not consistently reflect basic anatomical information. Moreover, synthetic modifications -- such as substituting "left" for "right" -- do not substantially influence highlights. Simple techniques such as allowing the model to opt out of attending to the image and few-shot finetuning show promise in terms of their ability to improve alignments with very little or no supervision.
Query-Focused EHR Summarization to Aid Imaging Diagnosis
Apr 26, 2020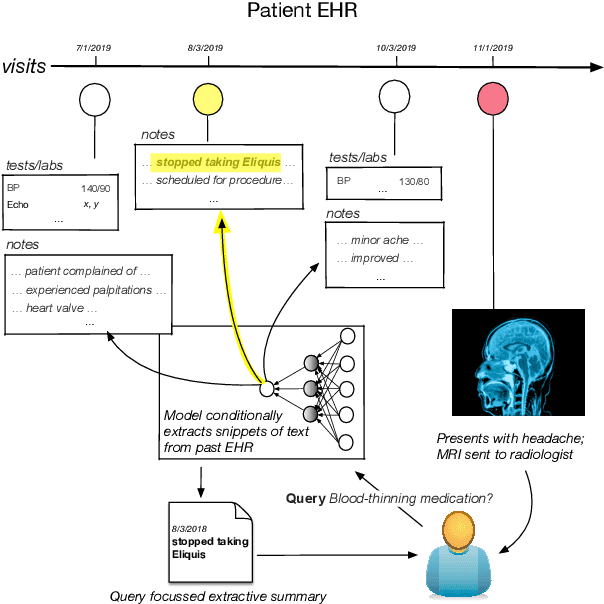
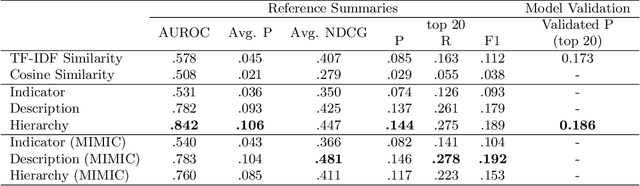


Electronic Health Records (EHRs) provide vital contextual information to radiologists and other physicians when making a diagnosis. Unfortunately, because a given patient's record may contain hundreds of notes and reports, identifying relevant information within these in the short time typically allotted to a case is very difficult. We propose and evaluate models that extract relevant text snippets from patient records to provide a rough case summary intended to aid physicians considering one or more diagnoses. This is hard because direct supervision (i.e., physician annotations of snippets relevant to specific diagnoses in medical records) is prohibitively expensive to collect at scale. We propose a distantly supervised strategy in which we use groups of International Classification of Diseases (ICD) codes observed in 'future' records as noisy proxies for 'downstream' diagnoses. Using this we train a transformer-based neural model to perform extractive summarization conditioned on potential diagnoses. This model defines an attention mechanism that is conditioned on potential diagnoses (queries) provided by the diagnosing physician. We train (via distant supervision) and evaluate variants of this model on EHR data from Brigham and Women's Hospital in Boston and MIMIC-III (the latter to facilitate reproducibility). Evaluations performed by radiologists demonstrate that these distantly supervised models yield better extractive summaries than do unsupervised approaches. Such models may aid diagnosis by identifying sentences in past patient reports that are clinically relevant to a potential diagnosis.