 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgePre-examinations Improve Automated Metastases Detection on Cranial MRI
Mar 13, 2024Materials and methods: First, a dual-time approach was assessed, for which the CNN was provided sequences of the MRI that initially depicted new MM (diagnosis MRI) as well as of a prediagnosis MRI: inclusion of only contrast-enhanced T1-weighted images (CNNdual_ce) was compared with inclusion of also the native T1-weighted images, T2-weighted images, and FLAIR sequences of both time points (CNNdual_all).Second, results were compared with the corresponding single time approaches, in which the CNN was provided exclusively the respective sequences of the diagnosis MRI.Casewise diagnostic performance parameters were calculated from 5-fold cross-validation. Results: In total, 94 cases with 494 MMs were included. Overall, the highest diagnostic performance was achieved by inclusion of only the contrast-enhanced T1-weighted images of the diagnosis and of a prediagnosis MRI (CNNdual_ce, sensitivity = 73%, PPV = 25%, F1-score = 36%). Using exclusively contrast-enhanced T1-weighted images as input resulted in significantly less false-positives (FPs) compared with inclusion of further sequences beyond contrast-enhanced T1-weighted images (FPs = 5/7 for CNNdual_ce/CNNdual_all, P < 1e-5). Comparison of contrast-enhanced dual and mono time approaches revealed that exclusion of prediagnosis MRI significantly increased FPs (FPs = 5/10 for CNNdual_ce/CNNce, P < 1e-9).Approaches with only native sequences were clearly inferior to CNNs that were provided contrast-enhanced sequences. Conclusions: Automated MM detection on contrast-enhanced T1-weighted images performed with high sensitivity. Frequent FPs due to artifacts and vessels were significantly reduced by additional inclusion of prediagnosis MRI, but not by inclusion of further sequences beyond contrast-enhanced T1-weighted images. Future studies might investigate different change detection architectures for computer-aided detection.
Revealing Hidden Potentials of the q-Space Signal in Breast Cancer
May 22, 2017
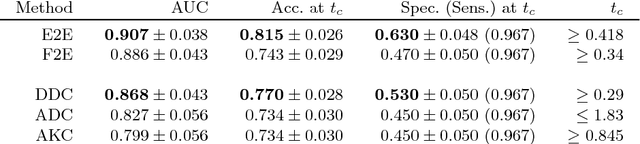
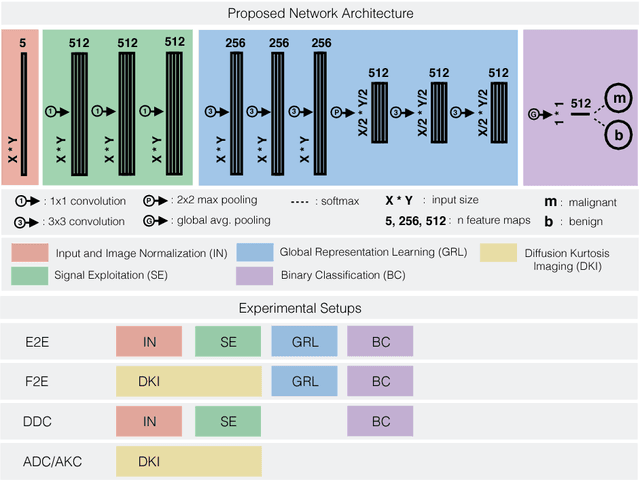
Mammography screening for early detection of breast lesions currently suffers from high amounts of false positive findings, which result in unnecessary invasive biopsies. Diffusion-weighted MR images (DWI) can help to reduce many of these false-positive findings prior to biopsy. Current approaches estimate tissue properties by means of quantitative parameters taken from generative, biophysical models fit to the q-space encoded signal under certain assumptions regarding noise and spatial homogeneity. This process is prone to fitting instability and partial information loss due to model simplicity. We reveal unexplored potentials of the signal by integrating all data processing components into a convolutional neural network (CNN) architecture that is designed to propagate clinical target information down to the raw input images. This approach enables simultaneous and target-specific optimization of image normalization, signal exploitation, global representation learning and classification. Using a multicentric data set of 222 patients, we demonstrate that our approach significantly improves clinical decision making with respect to the current state of the art.