 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeA Deployed Online Reinforcement Learning Algorithm In An Oral Health Clinical Trial
Sep 03, 2024



Dental disease is a prevalent chronic condition associated with substantial financial burden, personal suffering, and increased risk of systemic diseases. Despite widespread recommendations for twice-daily tooth brushing, adherence to recommended oral self-care behaviors remains sub-optimal due to factors such as forgetfulness and disengagement. To address this, we developed Oralytics, a mHealth intervention system designed to complement clinician-delivered preventative care for marginalized individuals at risk for dental disease. Oralytics incorporates an online reinforcement learning algorithm to determine optimal times to deliver intervention prompts that encourage oral self-care behaviors. We have deployed Oralytics in a registered clinical trial. The deployment required careful design to manage challenges specific to the clinical trials setting in the U.S. In this paper, we (1) highlight key design decisions of the RL algorithm that address these challenges and (2) conduct a re-sampling analysis to evaluate algorithm design decisions. A second phase (randomized control trial) of Oralytics is planned to start in spring 2025.
Oralytics Reinforcement Learning Algorithm
Jun 19, 2024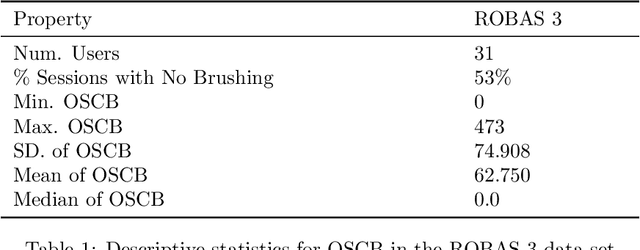
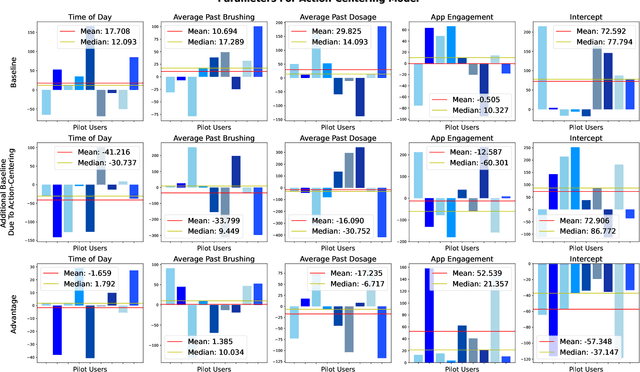
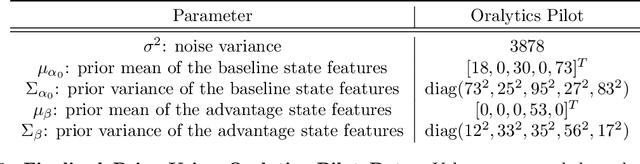

Dental disease is still one of the most common chronic diseases in the United States. While dental disease is preventable through healthy oral self-care behaviors (OSCB), this basic behavior is not consistently practiced. We have developed Oralytics, an online, reinforcement learning (RL) algorithm that optimizes the delivery of personalized intervention prompts to improve OSCB. In this paper, we offer a full overview of algorithm design decisions made using prior data, domain expertise, and experiments in a simulation test bed. The finalized RL algorithm was deployed in the Oralytics clinical trial, conducted from fall 2023 to summer 2024.
Monitoring Fidelity of Online Reinforcement Learning Algorithms in Clinical Trials
Feb 26, 2024
Online reinforcement learning (RL) algorithms offer great potential for personalizing treatment for participants in clinical trials. However, deploying an online, autonomous algorithm in the high-stakes healthcare setting makes quality control and data quality especially difficult to achieve. This paper proposes algorithm fidelity as a critical requirement for deploying online RL algorithms in clinical trials. It emphasizes the responsibility of the algorithm to (1) safeguard participants and (2) preserve the scientific utility of the data for post-trial analyses. We also present a framework for pre-deployment planning and real-time monitoring to help algorithm developers and clinical researchers ensure algorithm fidelity. To illustrate our framework's practical application, we present real-world examples from the Oralytics clinical trial. Since Spring 2023, this trial successfully deployed an autonomous, online RL algorithm to personalize behavioral interventions for participants at risk for dental disease.
Non-Stationary Latent Auto-Regressive Bandits
Feb 05, 2024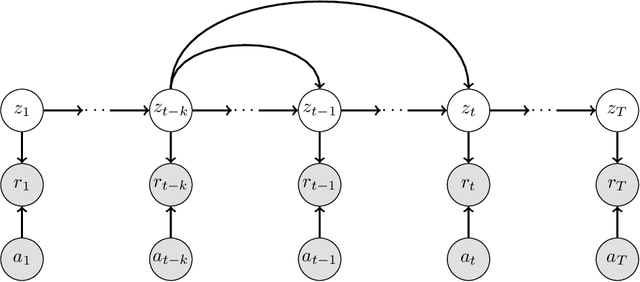
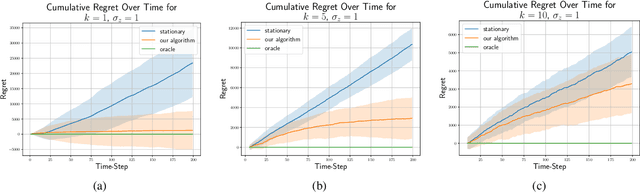
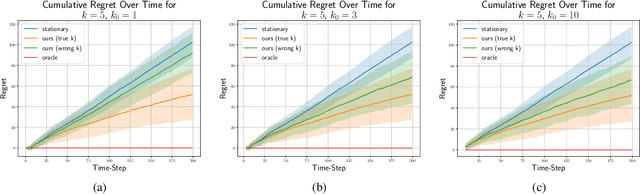
We consider the stochastic multi-armed bandit problem with non-stationary rewards. We present a novel formulation of non-stationarity in the environment where changes in the mean reward of the arms over time are due to some unknown, latent, auto-regressive (AR) state of order $k$. We call this new environment the latent AR bandit. Different forms of the latent AR bandit appear in many real-world settings, especially in emerging scientific fields such as behavioral health or education where there are few mechanistic models of the environment. If the AR order $k$ is known, we propose an algorithm that achieves $\tilde{O}(k\sqrt{T})$ regret in this setting. Empirically, our algorithm outperforms standard UCB across multiple non-stationary environments, even if $k$ is mis-specified.
Reward Design For An Online Reinforcement Learning Algorithm Supporting Oral Self-Care
Aug 15, 2022
Dental disease is one of the most common chronic diseases despite being largely preventable. However, professional advice on optimal oral hygiene practices is often forgotten or abandoned by patients. Therefore patients may benefit from timely and personalized encouragement to engage in oral self-care behaviors. In this paper, we develop an online reinforcement learning (RL) algorithm for use in optimizing the delivery of mobile-based prompts to encourage oral hygiene behaviors. One of the main challenges in developing such an algorithm is ensuring that the algorithm considers the impact of the current action on the effectiveness of future actions (i.e., delayed effects), especially when the algorithm has been made simple in order to run stably and autonomously in a constrained, real-world setting (i.e., highly noisy, sparse data). We address this challenge by designing a quality reward which maximizes the desired health outcome (i.e., high-quality brushing) while minimizing user burden. We also highlight a procedure for optimizing the hyperparameters of the reward by building a simulation environment test bed and evaluating candidates using the test bed. The RL algorithm discussed in this paper will be deployed in Oralytics, an oral self-care app that provides behavioral strategies to boost patient engagement in oral hygiene practices.
Designing Reinforcement Learning Algorithms for Digital Interventions: Pre-implementation Guidelines
Jun 08, 2022



Online reinforcement learning (RL) algorithms are increasingly used to personalize digital interventions in the fields of mobile health and online education. Common challenges in designing and testing an RL algorithm in these settings include ensuring the RL algorithm can learn and run stably under real-time constraints, and accounting for the complexity of the environment, e.g., a lack of accurate mechanistic models for the user dynamics. To guide how one can tackle these challenges, we extend the PCS (Predictability, Computability, Stability) framework, a data science framework that incorporates best practices from machine learning and statistics in supervised learning (Yu and Kumbier, 2020), to the design of RL algorithms for the digital interventions setting. Further, we provide guidelines on how to design simulation environments, a crucial tool for evaluating RL candidate algorithms using the PCS framework. We illustrate the use of the PCS framework for designing an RL algorithm for Oralytics, a mobile health study aiming to improve users' tooth-brushing behaviors through the personalized delivery of intervention messages. Oralytics will go into the field in late 2022.
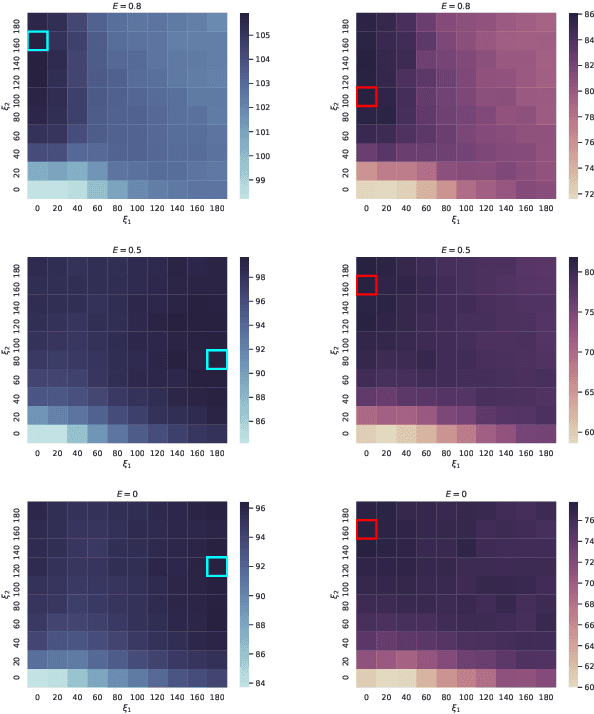
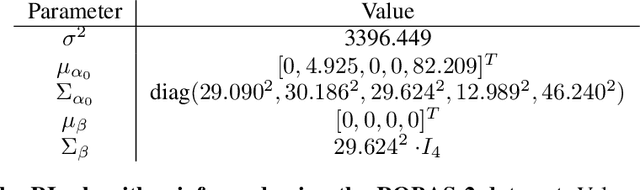
Discrepancies in Epidemiological Modeling of Aggregated Heterogeneous Data
Jun 20, 2021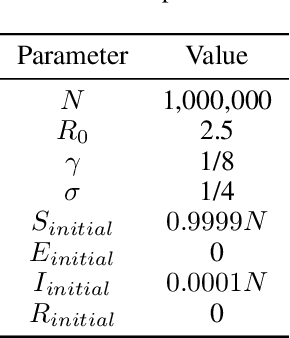
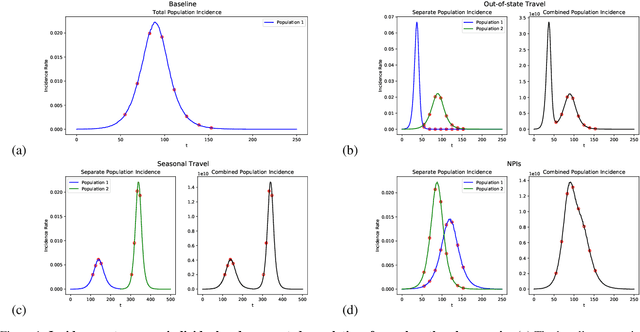

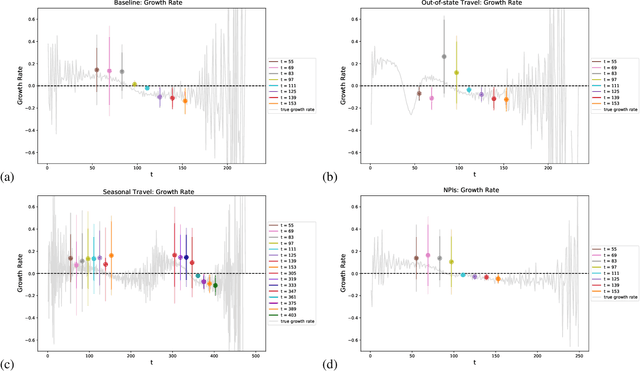
Within epidemiological modeling, the majority of analyses assume a single epidemic process for generating ground-truth data. However, this assumed data generation process can be unrealistic, since data sources for epidemics are often aggregated across geographic regions and communities. As a result, state-of-the-art models for estimating epidemiological parameters, e.g.~transmission rates, can be inappropriate when faced with complex systems. Our work empirically demonstrates some limitations of applying epidemiological models to aggregated datasets. We generate three complex outbreak scenarios by combining incidence curves from multiple epidemics that are independently simulated via SEIR models with different sets of parameters. Using these scenarios, we assess the robustness of a state-of-the-art Bayesian inference method that estimates the epidemic trajectory from viral load surveillance data. We evaluate two data-generating models within this Bayesian inference framework: a simple exponential growth model and a highly flexible Gaussian process prior model. Our results show that both models generate accurate transmission rate estimates for the combined incidence curve at the cost of generating biased estimates for each underlying epidemic, reflecting highly heterogeneous underlying population dynamics. The exponential growth model, while interpretable, is unable to capture the complexity of the underlying epidemics. With sufficient surveillance data, the Gaussian process prior model captures the shape of complex trajectories, but is imprecise for periods of low data coverage. Thus, our results highlight the potential pitfalls of neglecting complexity and heterogeneity in the data generation process, which can mask underlying location- and population-specific epidemic dynamics.