 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeMotion Artifacts Correction from Single-Channel EEG and fNIRS Signals using Novel Wavelet Packet Decomposition in Combination with Canonical Correlation Analysis
Apr 09, 2022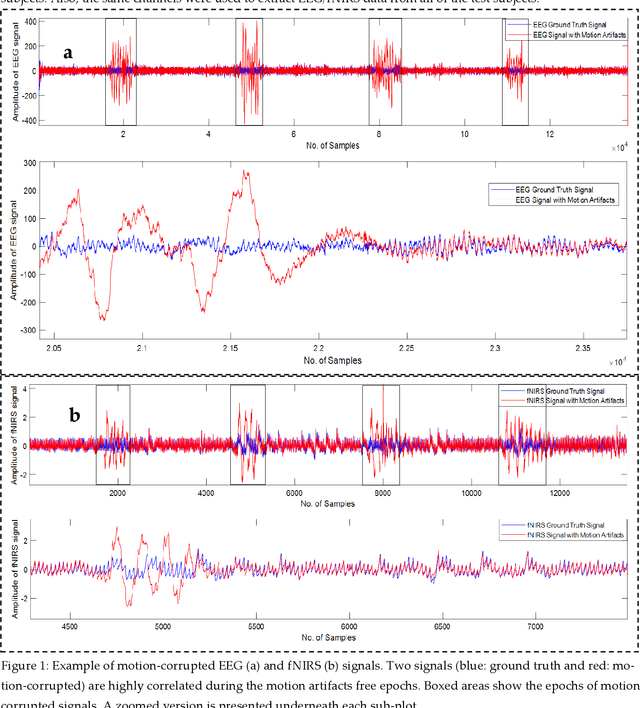
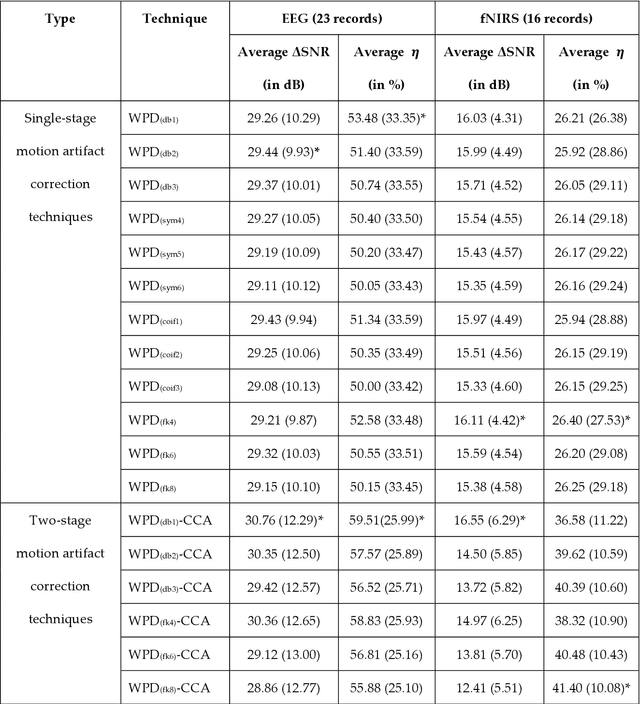
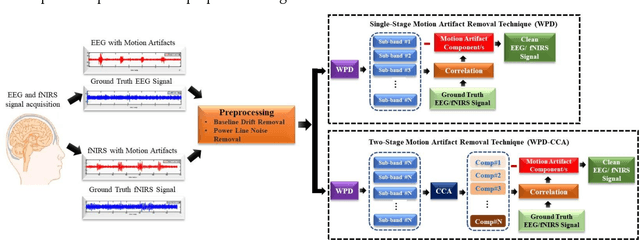
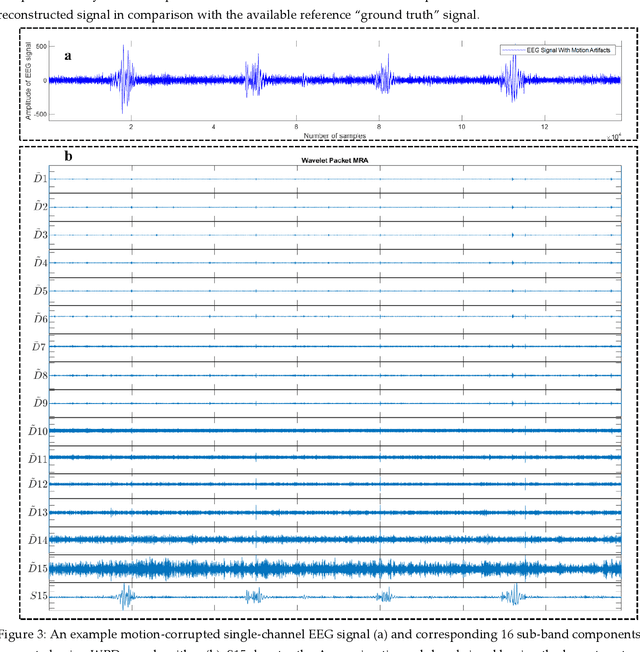
The electroencephalogram (EEG) and functional near-infrared spectroscopy (fNIRS) signals, highly non-stationary in nature, greatly suffers from motion artifacts while recorded using wearable sensors. This paper proposes two robust methods: i) Wavelet packet decomposition (WPD), and ii) WPD in combination with canonical correlation analysis (WPD-CCA), for motion artifact correction from single-channel EEG and fNIRS signals. The efficacy of these proposed techniques is tested using a benchmark dataset and the performance of the proposed methods is measured using two well-established performance matrices: i) Difference in the signal to noise ratio ({\Delta}SNR) and ii) Percentage reduction in motion artifacts ({\eta}). The proposed WPD-based single-stage motion artifacts correction technique produces the highest average {\Delta}SNR (29.44 dB) when db2 wavelet packet is incorporated whereas the greatest average {\eta} (53.48%) is obtained using db1 wavelet packet for all the available 23 EEG recordings. Our proposed two-stage motion artifacts correction technique i.e. the WPD-CCA method utilizing db1 wavelet packet has shown the best denoising performance producing an average {\Delta}SNR and {\eta} values of 30.76 dB and 59.51%, respectively for all the EEG recordings. On the other hand, the two-stage motion artifacts removal technique i.e. WPD-CCA has produced the best average {\Delta}SNR (16.55 dB, utilizing db1 wavelet packet) and largest average {\eta} (41.40%, using fk8 wavelet packet). The highest average {\Delta}SNR and {\eta} using single-stage artifacts removal techniques (WPD) are found as 16.11 dB and 26.40%, respectively for all the fNIRS signals using fk4 wavelet packet. In both EEG and fNIRS modalities, the percentage reduction in motion artifacts increases by 11.28% and 56.82%, respectively when two-stage WPD-CCA techniques are employed.
A Machine Learning Model for Early Detection of Diabetic Foot using Thermogram Images
Jun 27, 2021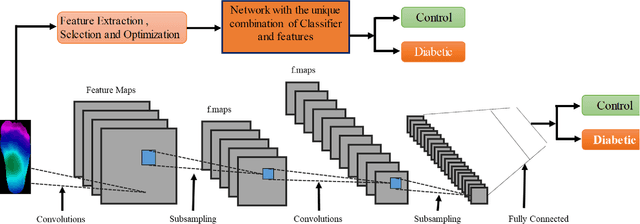
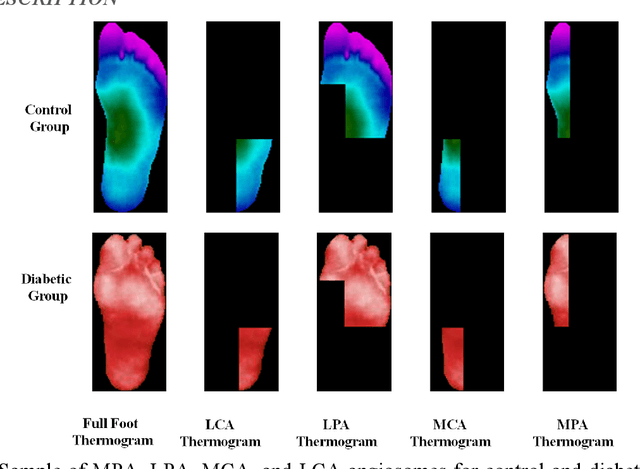
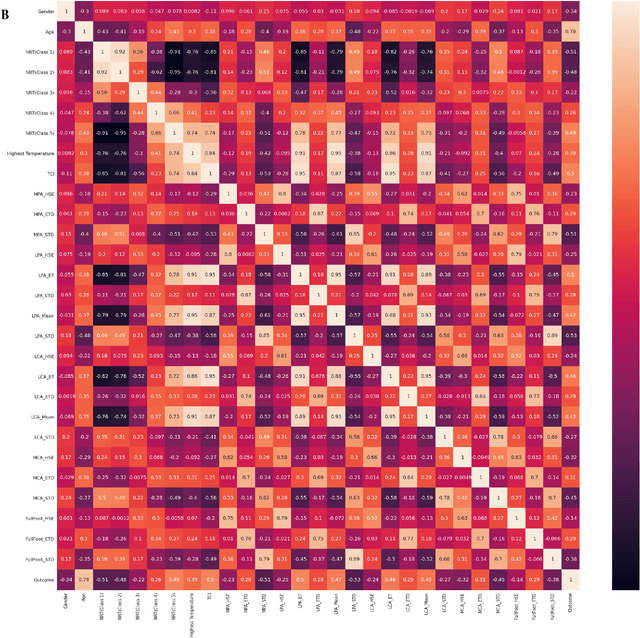
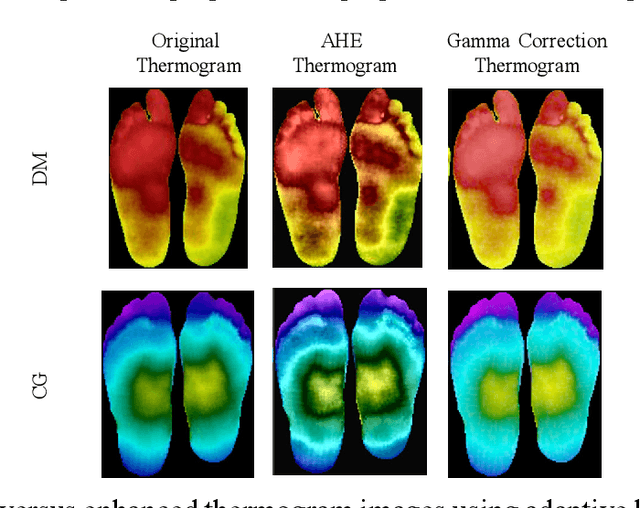
Diabetes foot ulceration (DFU) and amputation are a cause of significant morbidity. The prevention of DFU may be achieved by the identification of patients at risk of DFU and the institution of preventative measures through education and offloading. Several studies have reported that thermogram images may help to detect an increase in plantar temperature prior to DFU. However, the distribution of plantar temperature may be heterogeneous, making it difficult to quantify and utilize to predict outcomes. We have compared a machine learning-based scoring technique with feature selection and optimization techniques and learning classifiers to several state-of-the-art Convolutional Neural Networks (CNNs) on foot thermogram images and propose a robust solution to identify the diabetic foot. A comparatively shallow CNN model, MobilenetV2 achieved an F1 score of ~95% for a two-feet thermogram image-based classification and the AdaBoost Classifier used 10 features and achieved an F1 score of 97 %. A comparison of the inference time for the best-performing networks confirmed that the proposed algorithm can be deployed as a smartphone application to allow the user to monitor the progression of the DFU in a home setting.