 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeMotion Artifacts Correction from Single-Channel EEG and fNIRS Signals using Novel Wavelet Packet Decomposition in Combination with Canonical Correlation Analysis
Apr 09, 2022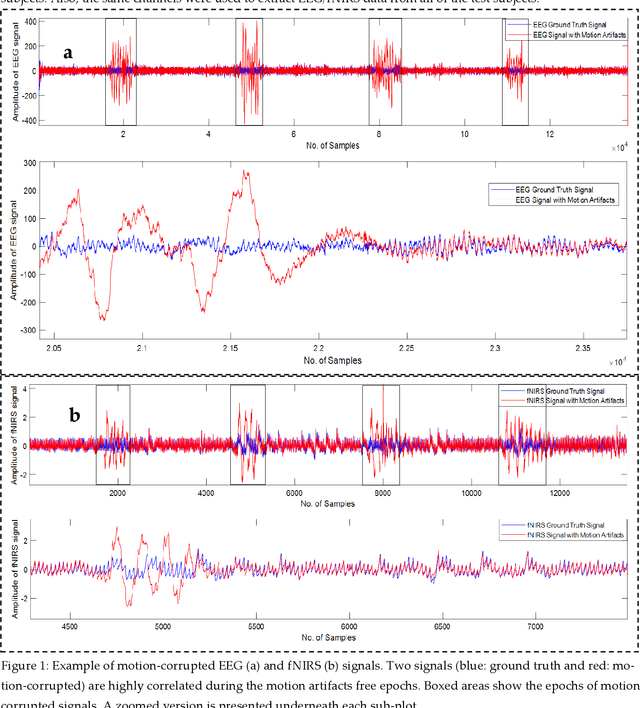
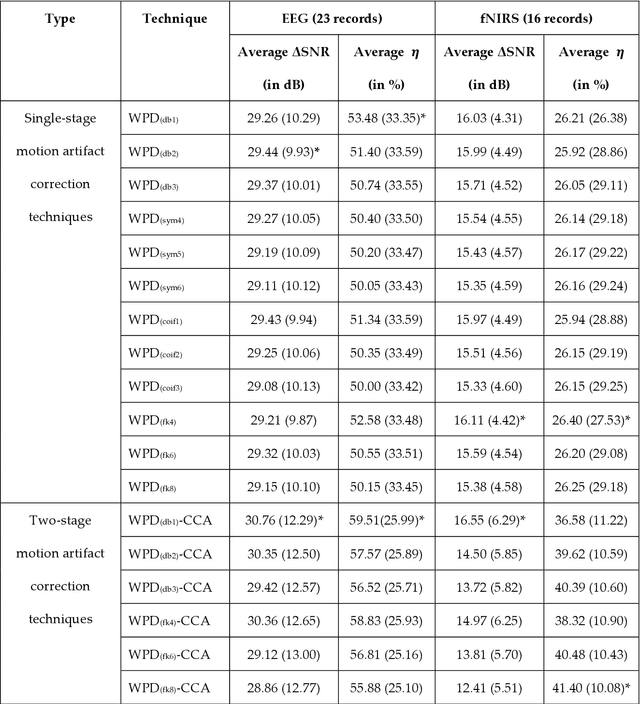
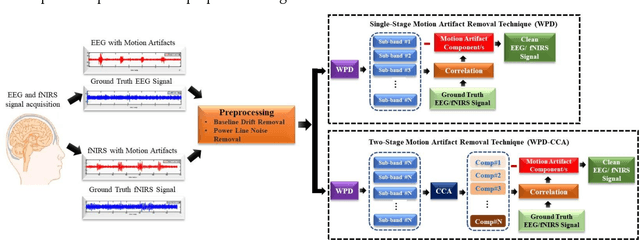
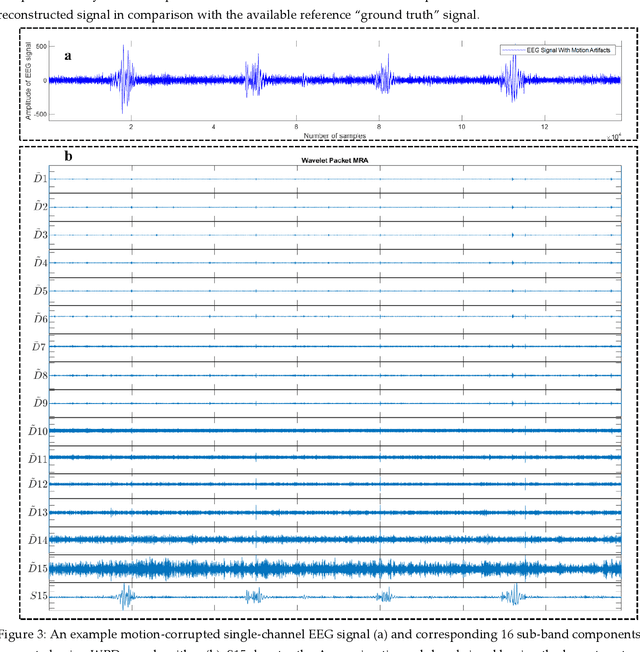
The electroencephalogram (EEG) and functional near-infrared spectroscopy (fNIRS) signals, highly non-stationary in nature, greatly suffers from motion artifacts while recorded using wearable sensors. This paper proposes two robust methods: i) Wavelet packet decomposition (WPD), and ii) WPD in combination with canonical correlation analysis (WPD-CCA), for motion artifact correction from single-channel EEG and fNIRS signals. The efficacy of these proposed techniques is tested using a benchmark dataset and the performance of the proposed methods is measured using two well-established performance matrices: i) Difference in the signal to noise ratio ({\Delta}SNR) and ii) Percentage reduction in motion artifacts ({\eta}). The proposed WPD-based single-stage motion artifacts correction technique produces the highest average {\Delta}SNR (29.44 dB) when db2 wavelet packet is incorporated whereas the greatest average {\eta} (53.48%) is obtained using db1 wavelet packet for all the available 23 EEG recordings. Our proposed two-stage motion artifacts correction technique i.e. the WPD-CCA method utilizing db1 wavelet packet has shown the best denoising performance producing an average {\Delta}SNR and {\eta} values of 30.76 dB and 59.51%, respectively for all the EEG recordings. On the other hand, the two-stage motion artifacts removal technique i.e. WPD-CCA has produced the best average {\Delta}SNR (16.55 dB, utilizing db1 wavelet packet) and largest average {\eta} (41.40%, using fk8 wavelet packet). The highest average {\Delta}SNR and {\eta} using single-stage artifacts removal techniques (WPD) are found as 16.11 dB and 26.40%, respectively for all the fNIRS signals using fk4 wavelet packet. In both EEG and fNIRS modalities, the percentage reduction in motion artifacts increases by 11.28% and 56.82%, respectively when two-stage WPD-CCA techniques are employed.
A machine learning-based severity prediction tool for diabetic sensorimotor polyneuropathy using Michigan neuropathy screening instrumentations
Mar 28, 2022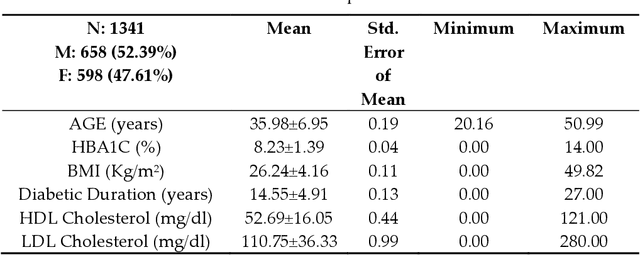
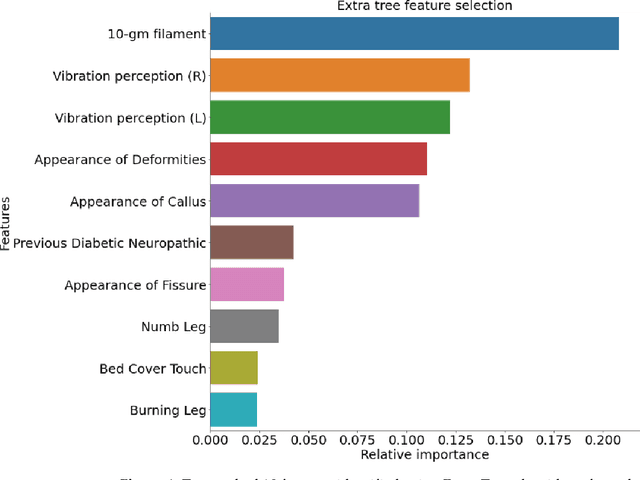
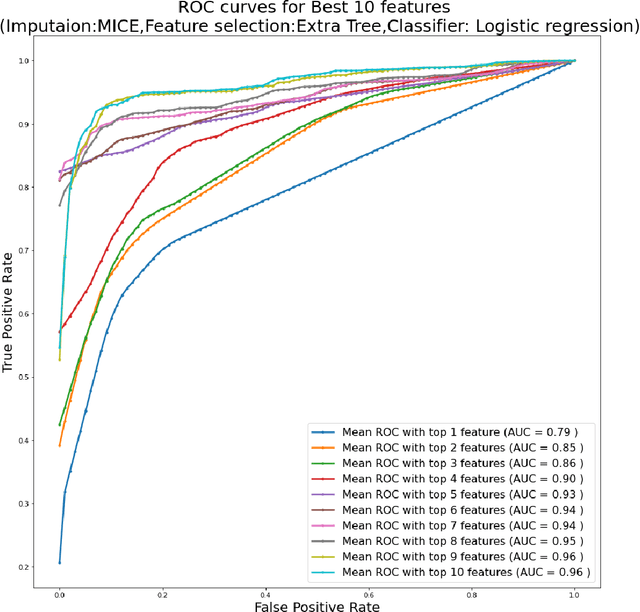
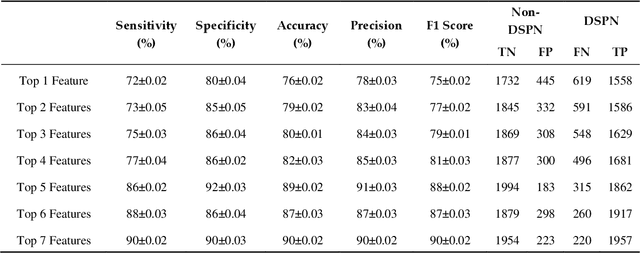
Background: Diabetic Sensorimotor polyneuropathy (DSPN) is a major long-term complication in diabetic patients associated with painful neuropathy, foot ulceration and amputation. The Michigan neuropathy screening instrument (MNSI) is one of the most common screening techniques for DSPN, however, it does not provide any direct severity grading system. Method: For designing and modelling the DSPN severity grading systems for MNSI, 19 years of data from Epidemiology of Diabetes Interventions and Complications (EDIC) clinical trials were used. MNSI variables and patient outcomes were investigated using machine learning tools to identify the features having higher association in DSPN identification. A multivariable logistic regression-based nomogram was generated and validated for DSPN severity grading. Results: The top-7 ranked features from MNSI: 10-gm filament, Vibration perception (R), Vibration perception (L), previous diabetic neuropathy, the appearance of deformities, appearance of callus and appearance of fissure were identified as key features for identifying DSPN using the extra tree model. The area under the curve (AUC) of the nomogram for the internal and external datasets were 0.9421 and 0.946, respectively. From the developed nomogram, the probability of having DSPN was predicted and a DSPN severity scoring system for MNSI was developed from the probability score. The model performance was validated on an independent dataset. Patients were stratified into four severity levels: absent, mild, moderate, and severe using a cut-off value of 10.5, 12.7 and 15 for a DSPN probability less than 50%, 75% to 90%, and above 90%, respectively. Conclusions: This study provides a simple, easy-to-use and reliable algorithm for defining the prognosis and management of patients with DSPN.