 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeMulti-State-Action Tokenisation in Decision Transformers for Multi-Discrete Action Spaces
Jul 01, 2024



Decision Transformers, in their vanilla form, struggle to perform on image-based environments with multi-discrete action spaces. Although enhanced Decision Transformer architectures have been developed to improve performance, these methods have not specifically addressed this problem of multi-discrete action spaces which hampers existing Decision Transformer architectures from learning good representations. To mitigate this, we propose Multi-State Action Tokenisation (M-SAT), an approach for tokenising actions in multi-discrete action spaces that enhances the model's performance in such environments. Our approach involves two key changes: disentangling actions to the individual action level and tokenising the actions with auxiliary state information. These two key changes also improve individual action level interpretability and visibility within the attention layers. We demonstrate the performance gains of M-SAT on challenging ViZDoom environments with multi-discrete action spaces and image-based state spaces, including the Deadly Corridor and My Way Home scenarios, where M-SAT outperforms the baseline Decision Transformer without any additional data or heavy computational overheads. Additionally, we find that removing positional encoding does not adversely affect M-SAT's performance and, in some cases, even improves it.
A Conservative Q-Learning approach for handling distribution shift in sepsis treatment strategies
Mar 25, 2022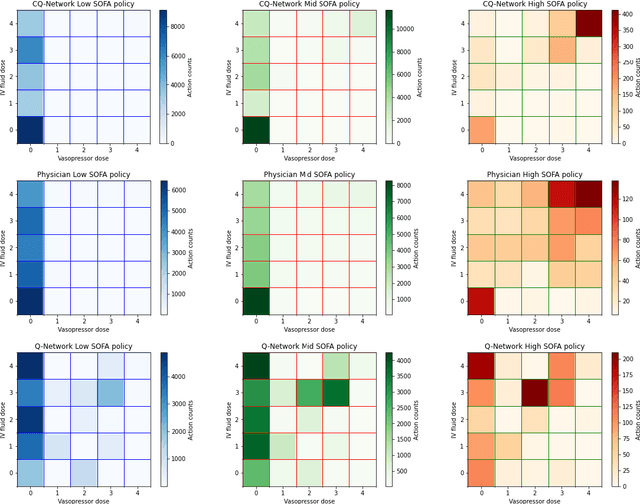
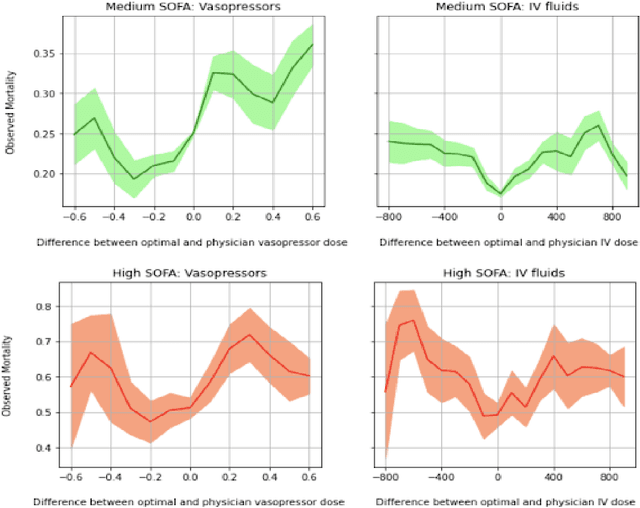
Sepsis is a leading cause of mortality and its treatment is very expensive. Sepsis treatment is also very challenging because there is no consensus on what interventions work best and different patients respond very differently to the same treatment. Deep Reinforcement Learning methods can be used to come up with optimal policies for treatment strategies mirroring physician actions. In the healthcare scenario, the available data is mostly collected offline with no interaction with the environment, which necessitates the use of offline RL techniques. The Offline RL paradigm suffers from action distribution shifts which in turn negatively affects learning an optimal policy for the treatment. In this work, a Conservative-Q Learning (CQL) algorithm is used to mitigate this shift and its corresponding policy reaches closer to the physicians policy than conventional deep Q Learning. The policy learned could help clinicians in Intensive Care Units to make better decisions while treating septic patients and improve survival rate.