 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeRuntime data center temperature prediction using Grammatical Evolution techniques
Nov 11, 2022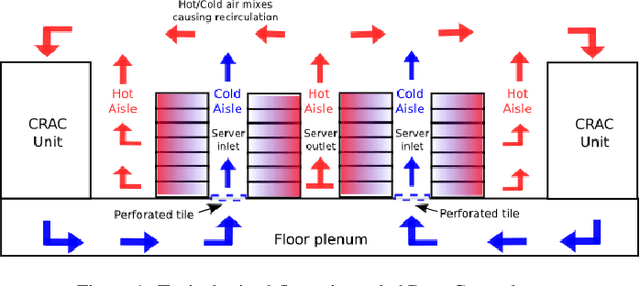


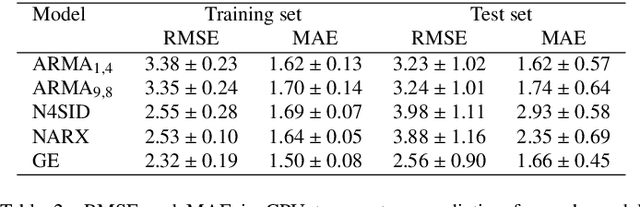
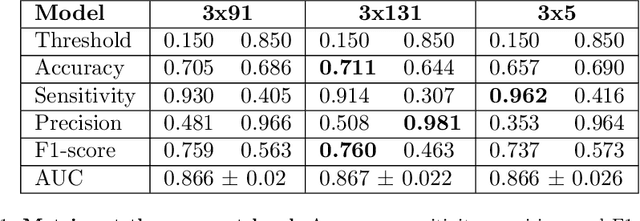
Data Centers are huge power consumers, both because of the energy required for computation and the cooling needed to keep servers below thermal redlining. The most common technique to minimize cooling costs is increasing data room temperature. However, to avoid reliability issues, and to enhance energy efficiency, there is a need to predict the temperature attained by servers under variable cooling setups. Due to the complex thermal dynamics of data rooms, accurate runtime data center temperature prediction has remained as an important challenge. By using Gramatical Evolution techniques, this paper presents a methodology for the generation of temperature models for data centers and the runtime prediction of CPU and inlet temperature under variable cooling setups. As opposed to time costly Computational Fluid Dynamics techniques, our models do not need specific knowledge about the problem, can be used in arbitrary data centers, re-trained if conditions change and have negligible overhead during runtime prediction. Our models have been trained and tested by using traces from real Data Center scenarios. Our results show how we can fully predict the temperature of the servers in a data rooms, with prediction errors below 2 C and 0.5 C in CPU and server inlet temperature respectively.
Interpreting Deep Learning Models for Epileptic Seizure Detection on EEG signals
Dec 22, 2020


While Deep Learning (DL) is often considered the state-of-the art for Artificial Intelligence-based medical decision support, it remains sparsely implemented in clinical practice and poorly trusted by clinicians due to insufficient interpretability of neural network models. We have tackled this issue by developing interpretable DL models in the context of online detection of epileptic seizure, based on EEG signal. This has conditioned the preparation of the input signals, the network architecture, and the post-processing of the output in line with the domain knowledge. Specifically, we focused the discussion on three main aspects: 1) how to aggregate the classification results on signal segments provided by the DL model into a larger time scale, at the seizure-level; 2) what are the relevant frequency patterns learned in the first convolutional layer of different models, and their relation with the delta, theta, alpha, beta and gamma frequency bands on which the visual interpretation of EEG is based; and 3) the identification of the signal waveforms with larger contribution towards the ictal class, according to the activation differences highlighted using the DeepLIFT method. Results show that the kernel size in the first layer determines the interpretability of the extracted features and the sensitivity of the trained models, even though the final performance is very similar after post-processing. Also, we found that amplitude is the main feature leading to an ictal prediction, suggesting that a larger patient population would be required to learn more complex frequency patterns. Still, our methodology was successfully able to generalize patient inter-variability for the majority of the studied population with a classification F1-score of 0.873 and detecting 90% of the seizures.