 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeMachine learning and AI research for Patient Benefit: 20 Critical Questions on Transparency, Replicability, Ethics and Effectiveness
Dec 21, 2018Machine learning (ML), artificial intelligence (AI) and other modern statistical methods are providing new opportunities to operationalize previously untapped and rapidly growing sources of data for patient benefit. Whilst there is a lot of promising research currently being undertaken, the literature as a whole lacks: transparency; clear reporting to facilitate replicability; exploration for potential ethical concerns; and, clear demonstrations of effectiveness. There are many reasons for why these issues exist, but one of the most important that we provide a preliminary solution for here is the current lack of ML/AI- specific best practice guidance. Although there is no consensus on what best practice looks in this field, we believe that interdisciplinary groups pursuing research and impact projects in the ML/AI for health domain would benefit from answering a series of questions based on the important issues that exist when undertaking work of this nature. Here we present 20 questions that span the entire project life cycle, from inception, data analysis, and model evaluation, to implementation, as a means to facilitate project planning and post-hoc (structured) independent evaluation. By beginning to answer these questions in different settings, we can start to understand what constitutes a good answer, and we expect that the resulting discussion will be central to developing an international consensus framework for transparent, replicable, ethical and effective research in artificial intelligence (AI-TREE) for health.
Machine Learning in Falls Prediction; A cognition-based predictor of falls for the acute neurological in-patient population
Jul 05, 2016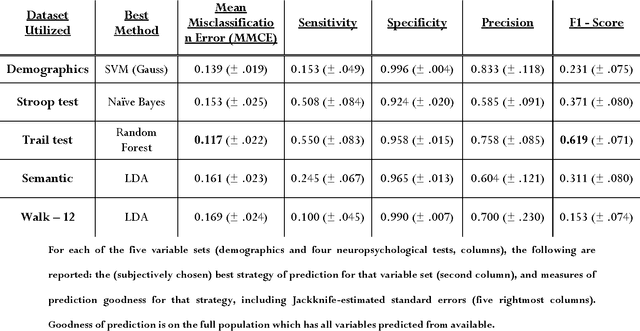
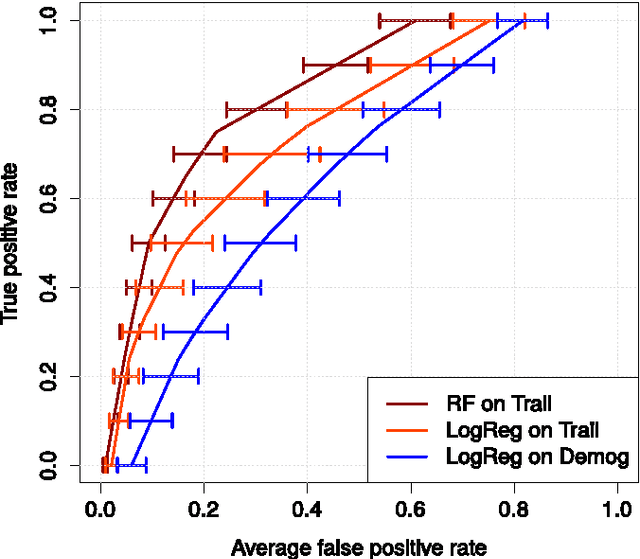
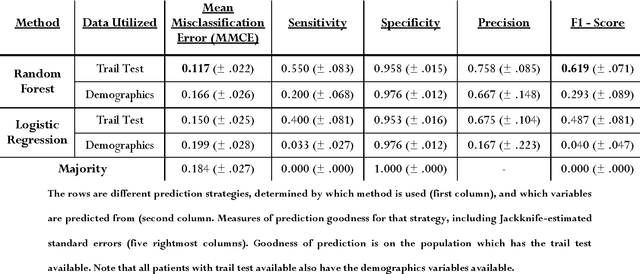
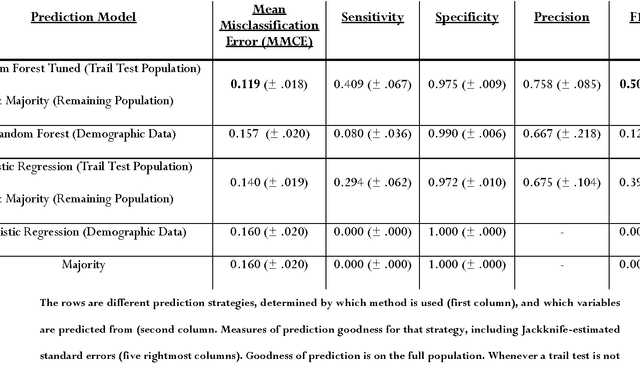
Background Information: Falls are associated with high direct and indirect costs, and significant morbidity and mortality for patients. Pathological falls are usually a result of a compromised motor system, and/or cognition. Very little research has been conducted on predicting falls based on this premise. Aims: To demonstrate that cognitive and motor tests can be used to create a robust predictive tool for falls. Methods: Three tests of attention and executive function (Stroop, Trail Making, and Semantic Fluency), a measure of physical function (Walk-12), a series of questions (concerning recent falls, surgery and physical function) and demographic information were collected from a cohort of 323 patients at a tertiary neurological center. The principal outcome was a fall during the in-patient stay (n = 54). Data-driven, predictive modelling was employed to identify the statistical modelling strategies which are most accurate in predicting falls, and which yield the most parsimonious models of clinical relevance. Results: The Trail test was identified as the best predictor of falls. Moreover, addition of any others variables, to the results of the Trail test did not improve the prediction (Wilcoxon signed-rank p < .001). The best statistical strategy for predicting falls was the random forest (Wilcoxon signed-rank p < .001), based solely on results of the Trail test. Tuning of the model results in the following optimized values: 68% (+- 7.7) sensitivity, 90% (+- 2.3) specificity, with a positive predictive value of 60%, when the relevant data is available. Conclusion: Predictive modelling has identified a simple yet powerful machine learning prediction strategy based on a single clinical test, the Trail test. Predictive evaluation shows this strategy to be robust, suggesting predictive modelling and machine learning as the standard for future predictive tools.