 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeCheXpedition: Investigating Generalization Challenges for Translation of Chest X-Ray Algorithms to the Clinical Setting
Mar 11, 2020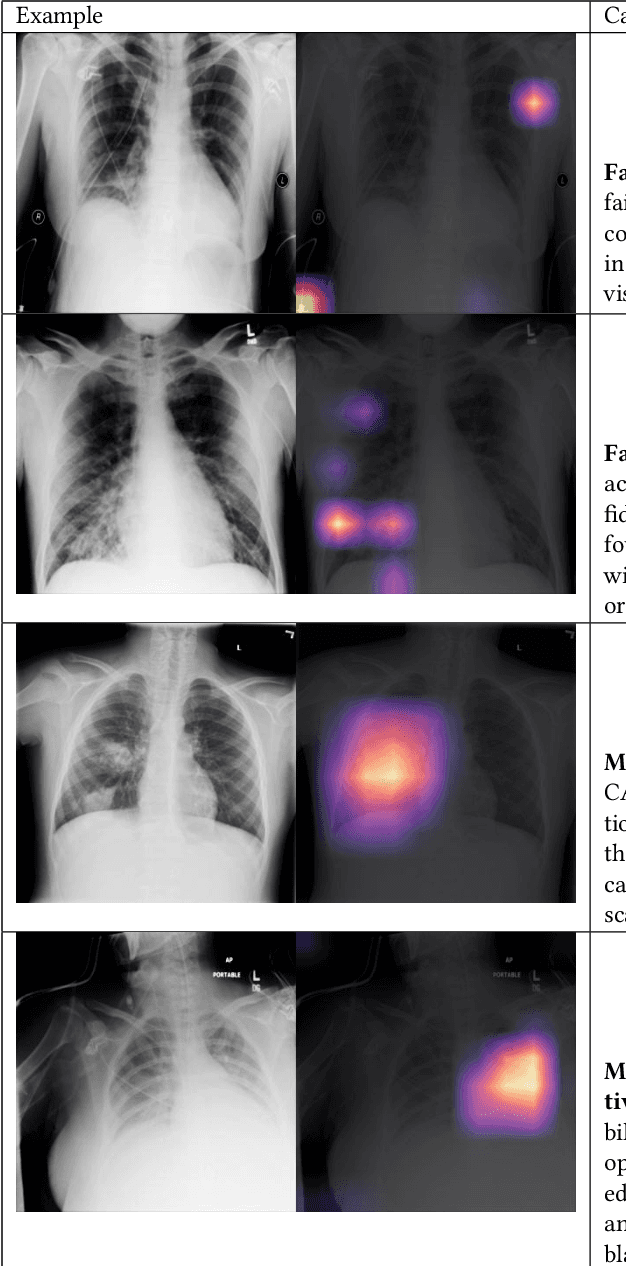
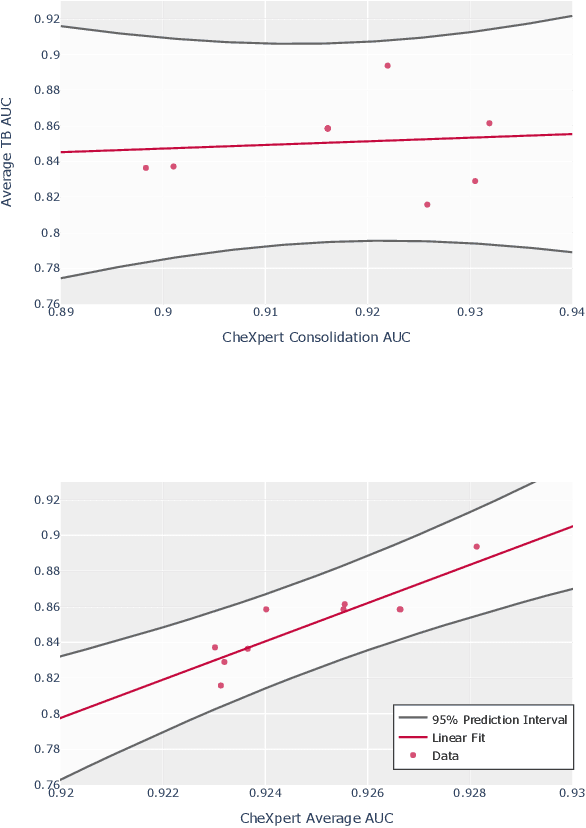
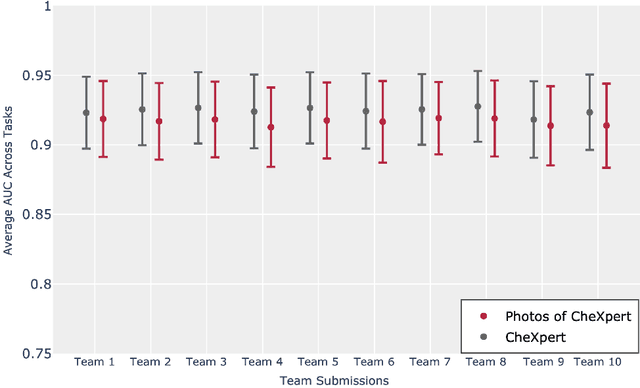
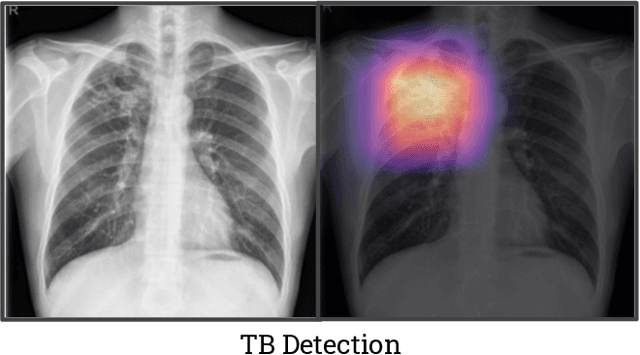
Although there have been several recent advances in the application of deep learning algorithms to chest x-ray interpretation, we identify three major challenges for the translation of chest x-ray algorithms to the clinical setting. We examine the performance of the top 10 performing models on the CheXpert challenge leaderboard on three tasks: (1) TB detection, (2) pathology detection on photos of chest x-rays, and (3) pathology detection on data from an external institution. First, we find that the top 10 chest x-ray models on the CheXpert competition achieve an average AUC of 0.851 on the task of detecting TB on two public TB datasets without fine-tuning or including the TB labels in training data. Second, we find that the average performance of the models on photos of x-rays (AUC = 0.916) is similar to their performance on the original chest x-ray images (AUC = 0.924). Third, we find that the models tested on an external dataset either perform comparably to or exceed the average performance of radiologists. We believe that our investigation will inform rapid translation of deep learning algorithms to safe and effective clinical decision support tools that can be validated prospectively with large impact studies and clinical trials.
Sepsis World Model: A MIMIC-based OpenAI Gym "World Model" Simulator for Sepsis Treatment
Dec 15, 2019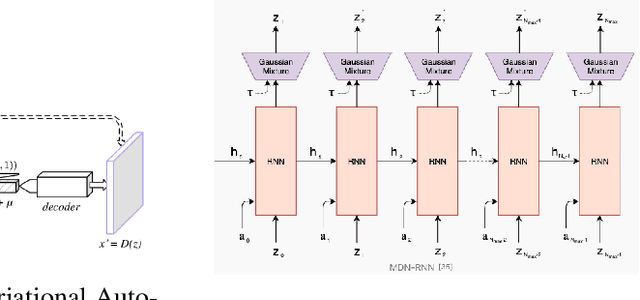
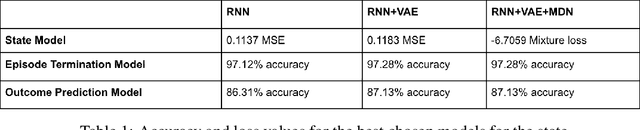
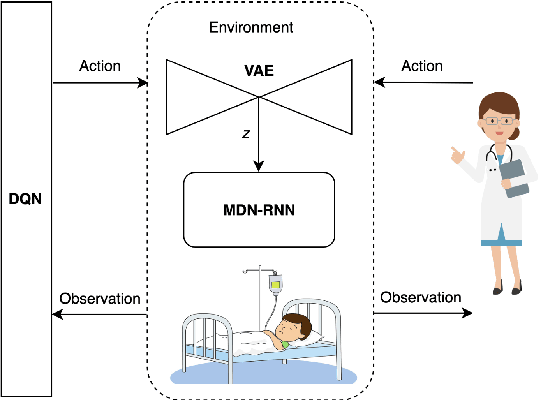
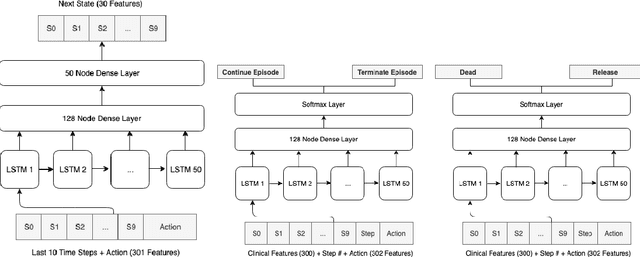
Sepsis is a life-threatening condition caused by the body's response to an infection. In order to treat patients with sepsis, physicians must control varying dosages of various antibiotics, fluids, and vasopressors based on a large number of variables in an emergency setting. In this project we employ a "world model" methodology to create a simulator that aims to predict the next state of a patient given a current state and treatment action. In doing so, we hope our simulator learns from a latent and less noisy representation of the EHR data. Using historical sepsis patient records from the MIMIC dataset, our method creates an OpenAI Gym simulator that leverages a Variational Auto-Encoder and a Mixture Density Network combined with a RNN (MDN-RNN) to model the trajectory of any sepsis patient in the hospital. To reduce the effects of noise, we sample from a generated distribution of next steps during simulation and have the option of introducing uncertainty into our simulator by controlling the "temperature" variable. It is worth noting that we do not have access to the ground truth for the best policy because we can only evaluate learned policies by real-world experimentation or expert feedback. Instead, we aim to study our simulator model's performance by evaluating the similarity between our environment's rollouts with the real EHR data and assessing its viability for learning a realistic policy for sepsis treatment using Deep Q-Learning.