 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeAutomated Assessment of Critical View of Safety in Laparoscopic Cholecystectomy
Sep 13, 2023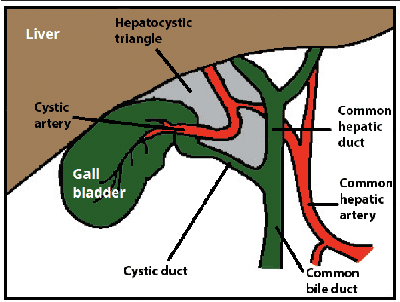
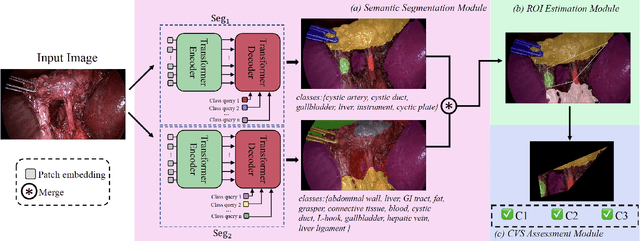
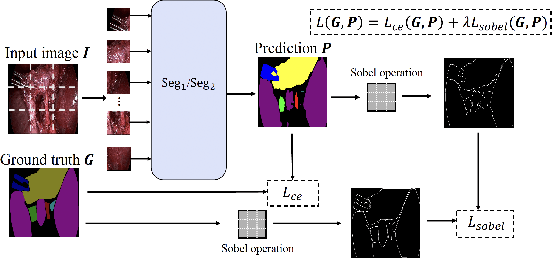
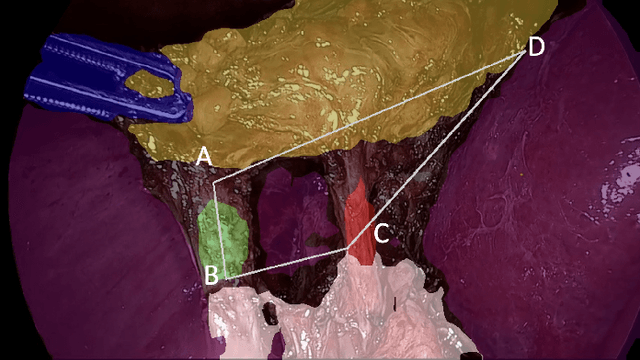
Cholecystectomy (gallbladder removal) is one of the most common procedures in the US, with more than 1.2M procedures annually. Compared with classical open cholecystectomy, laparoscopic cholecystectomy (LC) is associated with significantly shorter recovery period, and hence is the preferred method. However, LC is also associated with an increase in bile duct injuries (BDIs), resulting in significant morbidity and mortality. The primary cause of BDIs from LCs is misidentification of the cystic duct with the bile duct. Critical view of safety (CVS) is the most effective of safety protocols, which is said to be achieved during the surgery if certain criteria are met. However, due to suboptimal understanding and implementation of CVS, the BDI rates have remained stable over the last three decades. In this paper, we develop deep-learning techniques to automate the assessment of CVS in LCs. An innovative aspect of our research is on developing specialized learning techniques by incorporating domain knowledge to compensate for the limited training data available in practice. In particular, our CVS assessment process involves a fusion of two segmentation maps followed by an estimation of a certain region of interest based on anatomical structures close to the gallbladder, and then finally determination of each of the three CVS criteria via rule-based assessment of structural information. We achieved a gain of over 11.8% in mIoU on relevant classes with our two-stream semantic segmentation approach when compared to a single-model baseline, and 1.84% in mIoU with our proposed Sobel loss function when compared to a Transformer-based baseline model. For CVS criteria, we achieved up to 16% improvement and, for the overall CVS assessment, we achieved 5% improvement in balanced accuracy compared to DeepCVS under the same experiment settings.