 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeFirst do no harm: counterfactual objective functions for safe & ethical AI
Apr 27, 2022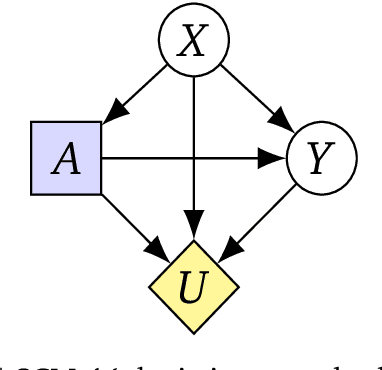
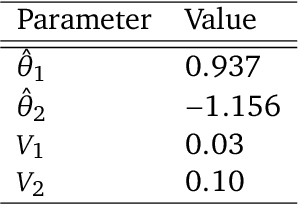
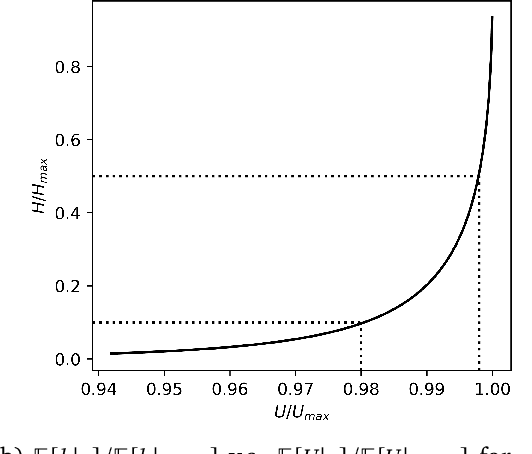
To act safely and ethically in the real world, agents must be able to reason about harm and avoid harmful actions. In this paper we develop the first statistical definition of harm and a framework for factoring harm into algorithmic decisions. We argue that harm is fundamentally a counterfactual quantity, and show that standard machine learning algorithms are guaranteed to pursue harmful policies in certain environments. To resolve this, we derive a family of counterfactual objective functions that robustly mitigate for harm. We demonstrate our approach with a statistical model for identifying optimal drug doses. While identifying optimal doses using the causal treatment effect results in harmful treatment decisions, our counterfactual algorithm identifies doses that are far less harmful without sacrificing efficacy. Our results show that counterfactual reasoning is a key ingredient for safe and ethical AI.
Learning medical triage from clinicians using Deep Q-Learning
Mar 28, 2020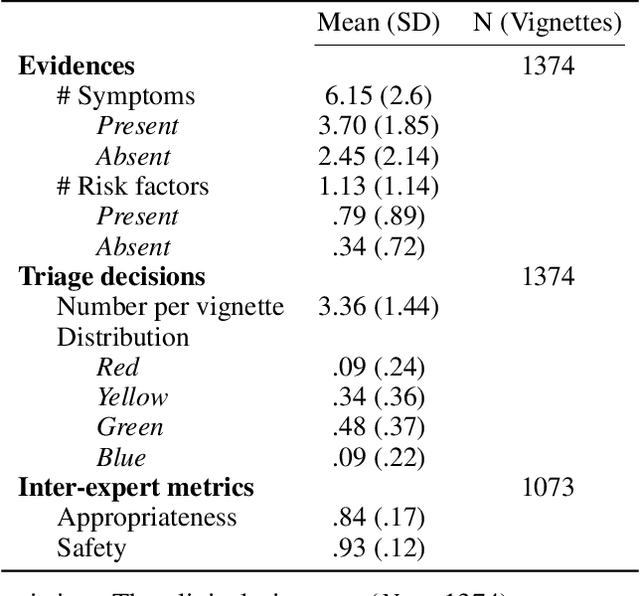
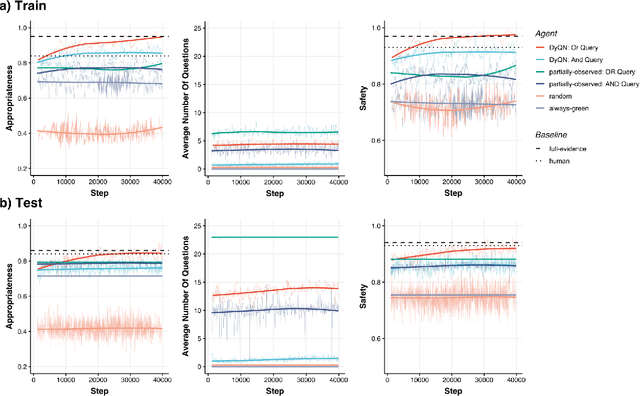
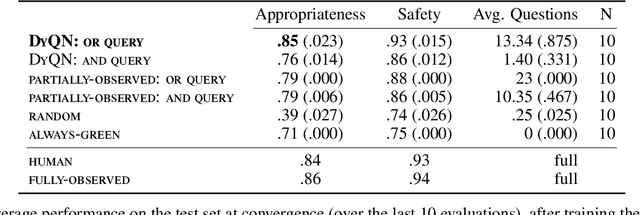
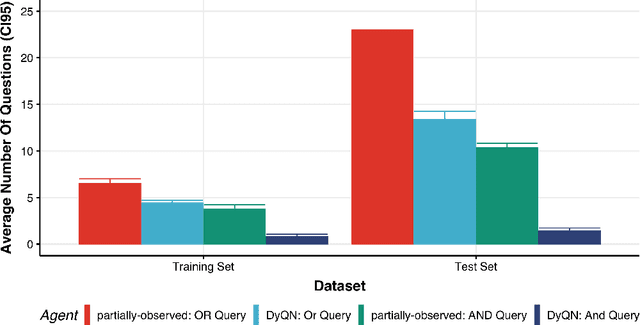
Medical Triage is of paramount importance to healthcare systems, allowing for the correct orientation of patients and allocation of the necessary resources to treat them adequately. While reliable decision-tree methods exist to triage patients based on their presentation, those trees implicitly require human inference and are not immediately applicable in a fully automated setting. On the other hand, learning triage policies directly from experts may correct for some of the limitations of hard-coded decision-trees. In this work, we present a Deep Reinforcement Learning approach (a variant of DeepQ-Learning) to triage patients using curated clinical vignettes. The dataset, consisting of 1374 clinical vignettes, was created by medical doctors to represent real-life cases. Each vignette is associated with an average of 3.8 expert triage decisions given by medical doctors relying solely on medical history. We show that this approach is on a par with human performance, yielding safe triage decisions in 94% of cases, and matching expert decisions in 85% of cases. The trained agent learns when to stop asking questions, acquires optimized decision policies requiring less evidence than supervised approaches, and adapts to the novelty of a situation by asking for more information. Overall, we demonstrate that a Deep Reinforcement Learning approach can learn effective medical triage policies directly from expert decisions, without requiring expert knowledge engineering. This approach is scalable and can be deployed in healthcare settings or geographical regions with distinct triage specifications, or where trained experts are scarce, to improve decision making in the early stage of care.