 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeDifferentiable Biomechanics for Markerless Motion Capture in Upper Limb Stroke Rehabilitation: A Comparison with Optical Motion Capture
Nov 22, 2024



Marker-based Optical Motion Capture (OMC) paired with biomechanical modeling is currently considered the most precise and accurate method for measuring human movement kinematics. However, combining differentiable biomechanical modeling with Markerless Motion Capture (MMC) offers a promising approach to motion capture in clinical settings, requiring only minimal equipment, such as synchronized webcams, and minimal effort for data collection. This study compares key kinematic outcomes from biomechanically modeled MMC and OMC data in 15 stroke patients performing the drinking task, a functional task recommended for assessing upper limb movement quality. We observed a high level of agreement in kinematic trajectories between MMC and OMC, as indicated by high correlations (median r above 0.95 for the majority of kinematic trajectories) and median RMSE values ranging from 2-5 degrees for joint angles, 0.04 m/s for end-effector velocity, and 6 mm for trunk displacement. Trial-to-trial biases between OMC and MMC were consistent within participant sessions, with interquartile ranges of bias around 1-3 degrees for joint angles, 0.01 m/s in end-effector velocity, and approximately 3mm for trunk displacement. Our findings indicate that our MMC for arm tracking is approaching the accuracy of marker-based methods, supporting its potential for use in clinical settings. MMC could provide valuable insights into movement rehabilitation in stroke patients, potentially enhancing the effectiveness of rehabilitation strategies.
Fusing uncalibrated IMUs and handheld smartphone video to reconstruct knee kinematics
May 27, 2024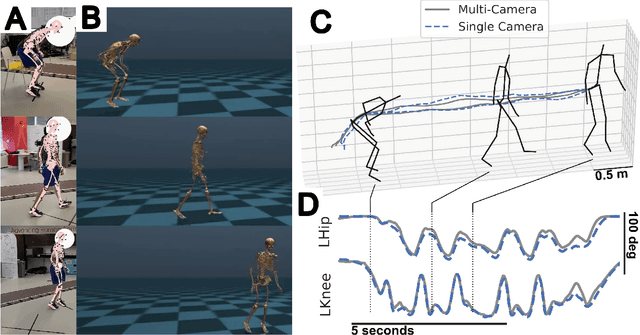
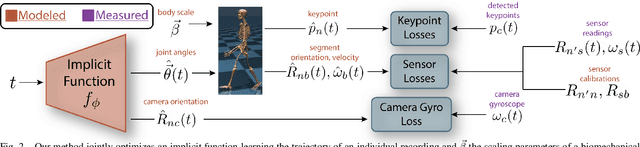
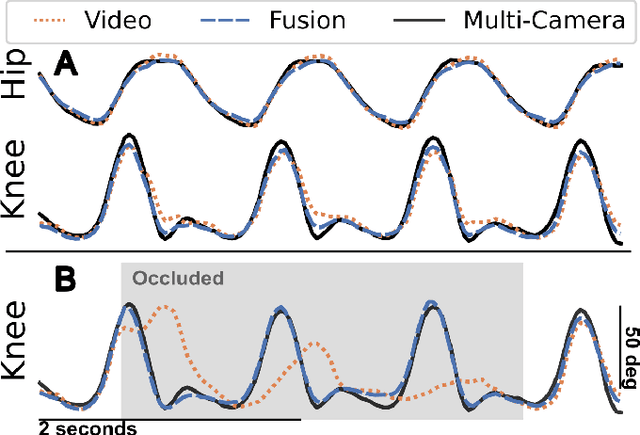
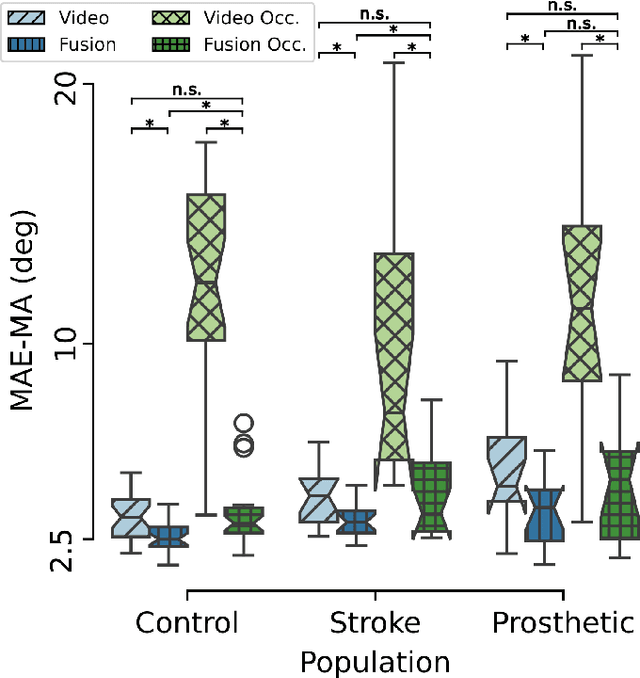
Video and wearable sensor data provide complementary information about human movement. Video provides a holistic understanding of the entire body in the world while wearable sensors provide high-resolution measurements of specific body segments. A robust method to fuse these modalities and obtain biomechanically accurate kinematics would have substantial utility for clinical assessment and monitoring. While multiple video-sensor fusion methods exist, most assume that a time-intensive, and often brittle, sensor-body calibration process has already been performed. In this work, we present a method to combine handheld smartphone video and uncalibrated wearable sensor data at their full temporal resolution. Our monocular, video-only, biomechanical reconstruction already performs well, with only several degrees of error at the knee during walking compared to markerless motion capture. Reconstructing from a fusion of video and wearable sensor data further reduces this error. We validate this in a mixture of people with no gait impairments, lower limb prosthesis users, and individuals with a history of stroke. We also show that sensor data allows tracking through periods of visual occlusion.
Self-Supervised Learning of Gait-Based Biomarkers
Jul 30, 2023



Markerless motion capture (MMC) is revolutionizing gait analysis in clinical settings by making it more accessible, raising the question of how to extract the most clinically meaningful information from gait data. In multiple fields ranging from image processing to natural language processing, self-supervised learning (SSL) from large amounts of unannotated data produces very effective representations for downstream tasks. However, there has only been limited use of SSL to learn effective representations of gait and movement, and it has not been applied to gait analysis with MMC. One SSL objective that has not been applied to gait is contrastive learning, which finds representations that place similar samples closer together in the learned space. If the learned similarity metric captures clinically meaningful differences, this could produce a useful representation for many downstream clinical tasks. Contrastive learning can also be combined with causal masking to predict future timesteps, which is an appealing SSL objective given the dynamical nature of gait. We applied these techniques to gait analyses performed with MMC in a rehabilitation hospital from a diverse clinical population. We find that contrastive learning on unannotated gait data learns a representation that captures clinically meaningful information. We probe this learned representation using the framework of biomarkers and show it holds promise as both a diagnostic and response biomarker, by showing it can accurately classify diagnosis from gait and is responsive to inpatient therapy, respectively. We ultimately hope these learned representations will enable predictive and prognostic gait-based biomarkers that can facilitate precision rehabilitation through greater use of MMC to quantify movement in rehabilitation.
* Accepted to Ambient Inteligence for Healthcare workshop at MICCAI 2023
Markerless Motion Capture and Biomechanical Analysis Pipeline
Mar 19, 2023



Markerless motion capture using computer vision and human pose estimation (HPE) has the potential to expand access to precise movement analysis. This could greatly benefit rehabilitation by enabling more accurate tracking of outcomes and providing more sensitive tools for research. There are numerous steps between obtaining videos to extracting accurate biomechanical results and limited research to guide many critical design decisions in these pipelines. In this work, we analyze several of these steps including the algorithm used to detect keypoints and the keypoint set, the approach to reconstructing trajectories for biomechanical inverse kinematics and optimizing the IK process. Several features we find important are: 1) using a recent algorithm trained on many datasets that produces a dense set of biomechanically-motivated keypoints, 2) using an implicit representation to reconstruct smooth, anatomically constrained marker trajectories for IK, 3) iteratively optimizing the biomechanical model to match the dense markers, 4) appropriate regularization of the IK process. Our pipeline makes it easy to obtain accurate biomechanical estimates of movement in a rehabilitation hospital.