 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeShape-based pose estimation for automatic standard views of the knee
May 26, 2023



Surgical treatment of complicated knee fractures is guided by real-time imaging using a mobile C-arm. Immediate and continuous control is achieved via 2D anatomy-specific standard views that correspond to a specific C-arm pose relative to the patient positioning, which is currently determined manually, following a trial-and-error approach at the cost of time and radiation dose. The characteristics of the standard views of the knee suggests that the shape information of individual bones could guide an automatic positioning procedure, reducing time and the amount of unnecessary radiation during C-arm positioning. To fully automate the C-arm positioning task during knee surgeries, we propose a complete framework that enables (1) automatic laterality and standard view classification and (2) automatic shape-based pose regression toward the desired standard view based on a single initial X-ray. A suitable shape representation is proposed to incorporate semantic information into the pose regression pipeline. The pipeline is designed to handle two distinct standard views simultaneously. Experiments were conducted to assess the performance of the proposed system on 3528 synthetic and 1386 real X-rays for the a.-p. and lateral standard. The view/laterality classificator resulted in an accuracy of 100\%/98\% on the simulated and 99\%/98\% on the real X-rays. The pose regression performance was $d\theta_{a.-p}=5.8\pm3.3\degree,\,d\theta_{lateral}=3.7\pm2.0\degree$ on the simulated data and $d\theta_{a.-p}=7.4\pm5.0\degree,\,d\theta_{lateral}=8.4\pm5.4\degree$ on the real data outperforming intensity-based pose regression.
Automatic Plane Adjustment of Orthopedic Intra-operative Flat Panel Detector CT-Volumes
Sep 15, 2021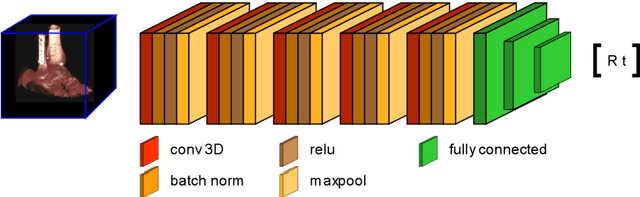


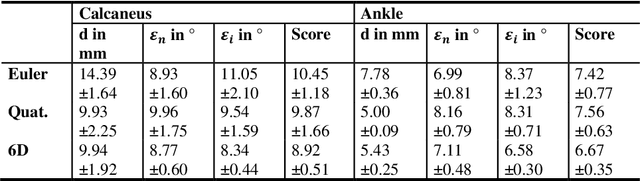
Purpose 3D acquisitions are often acquired to assess the result in orthopedic trauma surgery. With a mobile C-Arm system, these acquisitions can be performed intra-operatively. That reduces the number of required revision surgeries. However, due to the operation room setup, the acquisitions typically cannot be performed such that the acquired volumes are aligned to the anatomical regions. Thus, the multiplanar reconstructed (MPR) planes need to be adjusted manually during the review of the volume. In this paper, we present a detailed study of multi-task learning (MTL) regression networks to estimate the parameters of the MPR planes. Approach First, various mathematical descriptions for rotation, including Euler angle, quaternion, and matrix representation, are revised. Then, three different MTL network architectures based on the PoseNet are compared with a single task learning network. Results Using a matrix description rather than the Euler angle description, the accuracy of the regressed normals improves from $7.7^{\circ}$ to $7.3^{\circ}$ in the mean value for single anatomies. The multi-head approach improves the regression of the plane position from $7.4mm$ to $6.1mm$, while the orientation does not benefit from this approach. Conclusions The results show that a multi-head approach can lead to slightly better results than the individual tasks networks. The most important benefit of the MTL approach is that it is a single network for standard plane regression for all body regions with a reduced number of stored parameters.
Multi-task Localization and Segmentation for X-ray Guided Planning in Knee Surgery
Jul 24, 2019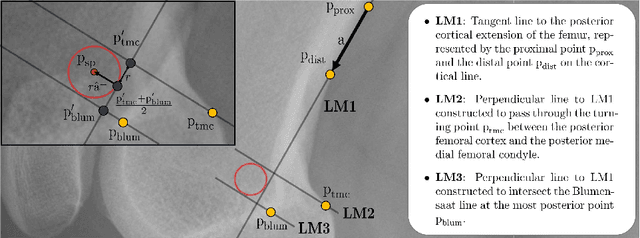


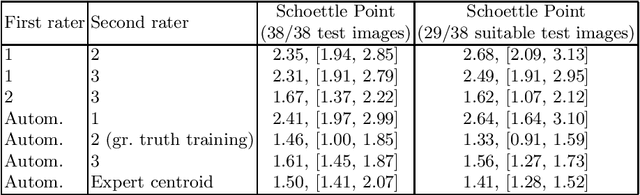
X-ray based measurement and guidance are commonly used tools in orthopaedic surgery to facilitate a minimally invasive workflow. Typically, a surgical planning is first performed using knowledge of bone morphology and anatomical landmarks. Information about bone location then serves as a prior for registration during overlay of the planning on intra-operative X-ray images. Performing these steps manually however is prone to intra-rater/inter-rater variability and increases task complexity for the surgeon. To remedy these issues, we propose an automatic framework for planning and subsequent overlay. We evaluate it on the example of femoral drill site planning for medial patellofemoral ligament reconstruction surgery. A deep multi-task stacked hourglass network is trained on 149 conventional lateral X-ray images to jointly localize two femoral landmarks, to predict a region of interest for the posterior femoral cortex tangent line, and to perform semantic segmentation of the femur, patella, tibia, and fibula with adaptive task complexity weighting. On 38 clinical test images the framework achieves a median localization error of 1.50 mm for the femoral drill site and mean IOU scores of 0.99, 0.97, 0.98, and 0.96 for the femur, patella, tibia, and fibula respectively. The demonstrated approach consistently performs surgical planning at expert-level precision without the need for manual correction.