 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeFast Nonparametric Conditional Independence Testing via Two-Stage Regression
Jun 16, 2026Constraint-based causal discovery relies on repeated conditional independence tests, but fast nonparametric tests often sacrifice calibration, especially when variables depend on the conditioning set through nonlinear relationships. We introduce BLITZ (Broad-to-Local Independence Testing via residualiZation), a nonparametric conditional independence test designed to run well under a second while maintaining the accuracy needed for the thousands of queries performed by constraint-based causal discovery algorithms. BLITZ first removes broad smooth dependence on the conditioning set using low-order polynomial regression, then applies a small nonlinear feature map and residualizes those features with shallow tree regressions. The resulting statistic tests residual cross-covariance, with a moment-matched chi-square approximation to the null distribution. We show theoretically that the two-stage design reduces the effective complexity faced by the tree residualizers, allowing shallow trees to control residual conditional-mean bias while avoiding excessive overfitting. In simulations, BLITZ provides better null calibration than fast kernel, random-feature, and regression-based competitors while remaining among the fastest methods tested. In causal discovery experiments on synthetic graphs and flow-cytometry data, BLITZ yields more reliable endpoint orientations among retained adjacencies and competitive structural recovery. These results suggest that broad-to-local residualization is a practical route to calibrated, scalable nonparametric conditional independence testing for causal discovery.
Extracting Root-Causal Brain Activity Driving Psychopathology from Resting State fMRI
Feb 06, 2026Neuroimaging studies of psychiatric disorders often correlate imaging patterns with diagnostic labels or composite symptom scores, yielding diffuse associations that obscure underlying mechanisms. We instead seek to identify root-causal maps -- localized BOLD disturbances that initiate pathological cascades -- and to link them selectively to symptom dimensions. We introduce a bilevel structural causal model that connects between-subject symptom structure to within-subject resting-state fMRI via independent latent sources with localized direct effects. Based on this model, we develop SOURCE (Symptom-Oriented Uncovering of Root-Causal Elements), a procedure that links interpretable symptom axes to a parsimonious set of localized drivers. Experiments show that SOURCE recovers localized maps consistent with root-causal BOLD drivers and increases interpretability and anatomical specificity relative to existing comparators.
A data-driven approach to discover and quantify systemic lupus erythematosus etiological heterogeneity from electronic health records
Jan 13, 2025Systemic lupus erythematosus (SLE) is a complex heterogeneous disease with many manifestational facets. We propose a data-driven approach to discover probabilistic independent sources from multimodal imperfect EHR data. These sources represent exogenous variables in the data generation process causal graph that estimate latent root causes of the presence of SLE in the health record. We objectively evaluated the sources against the original variables from which they were discovered by training supervised models to discriminate SLE from negative health records using a reduced set of labelled instances. We found 19 predictive sources with high clinical validity and whose EHR signatures define independent factors of SLE heterogeneity. Using the sources as input patient data representation enables models to provide with rich explanations that better capture the clinical reasons why a particular record is (not) an SLE case. Providers may be willing to trade patient-level interpretability for discrimination especially in challenging cases.
Unsupervised Discovery of Clinical Disease Signatures Using Probabilistic Independence
Feb 08, 2024



Insufficiently precise diagnosis of clinical disease is likely responsible for many treatment failures, even for common conditions and treatments. With a large enough dataset, it may be possible to use unsupervised machine learning to define clinical disease patterns more precisely. We present an approach to learning these patterns by using probabilistic independence to disentangle the imprint on the medical record of causal latent sources of disease. We inferred a broad set of 2000 clinical signatures of latent sources from 9195 variables in 269,099 Electronic Health Records. The learned signatures produced better discrimination than the original variables in a lung cancer prediction task unknown to the inference algorithm, predicting 3-year malignancy in patients with no history of cancer before a solitary lung nodule was discovered. More importantly, the signatures' greater explanatory power identified pre-nodule signatures of apparently undiagnosed cancer in many of those patients.
Why Do Clinical Probabilistic Models Fail To Transport Between Sites?
Nov 08, 2023The rising popularity of artificial intelligence in healthcare is highlighting the problem that a computational model achieving super-human clinical performance at its training sites may perform substantially worse at new sites. In this perspective, we present common sources for this failure to transport, which we divide into sources under the control of the experimenter and sources inherent to the clinical data-generating process. Of the inherent sources we look a little deeper into site-specific clinical practices that can affect the data distribution, and propose a potential solution intended to isolate the imprint of those practices on the data from the patterns of disease cause and effect that are the usual target of clinical models.
Counterfactual Formulation of Patient-Specific Root Causes of Disease
May 31, 2023Root causes of disease intuitively correspond to root vertices that increase the likelihood of a diagnosis. This description of a root cause nevertheless lacks the rigorous mathematical formulation needed for the development of computer algorithms designed to automatically detect root causes from data. Prior work defined patient-specific root causes of disease using an interventionalist account that only climbs to the second rung of Pearl's Ladder of Causation. In this theoretical piece, we climb to the third rung by proposing a counterfactual definition matching clinical intuition based on fixed factual data alone. We then show how to assign a root causal contribution score to each variable using Shapley values from explainable artificial intelligence. The proposed counterfactual formulation of patient-specific root causes of disease accounts for noisy labels, adapts to disease prevalence and admits fast computation without the need for counterfactual simulation.
Sample-Specific Root Causal Inference with Latent Variables
Oct 27, 2022Root causal analysis seeks to identify the set of initial perturbations that induce an unwanted outcome. In prior work, we defined sample-specific root causes of disease using exogenous error terms that predict a diagnosis in a structural equation model. We rigorously quantified predictivity using Shapley values. However, the associated algorithms for inferring root causes assume no latent confounding. We relax this assumption by permitting confounding among the predictors. We then introduce a corresponding procedure called Extract Errors with Latents (EEL) for recovering the error terms up to contamination by vertices on certain paths under the linear non-Gaussian acyclic model. EEL also identifies the smallest sets of dependent errors for fast computation of the Shapley values. The algorithm bypasses the hard problem of estimating the underlying causal graph in both cases. Experiments highlight the superior accuracy and robustness of EEL relative to its predecessors.
Identifying Patient-Specific Root Causes with the Heteroscedastic Noise Model
May 25, 2022
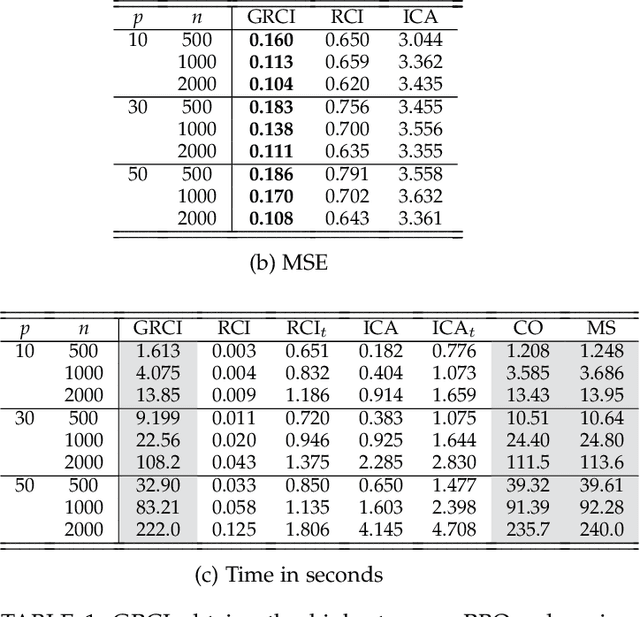

Complex diseases are caused by a multitude of factors that may differ between patients even within the same diagnostic category. A few underlying root causes may nevertheless initiate the development of disease within each patient. We therefore focus on identifying patient-specific root causes of disease, which we equate to the sample-specific predictivity of the exogenous error terms in a structural equation model. We generalize from the linear setting to the heteroscedastic noise model where $Y = m(X) + \varepsilon\sigma(X)$ with non-linear functions $m(X)$ and $\sigma(X)$ representing the conditional mean and mean absolute deviation, respectively. This model preserves identifiability but introduces non-trivial challenges that require a customized algorithm called Generalized Root Causal Inference (GRCI) to extract the error terms correctly. GRCI recovers patient-specific root causes more accurately than existing alternatives.
Identifying Patient-Specific Root Causes of Disease
May 23, 2022

Complex diseases are caused by a multitude of factors that may differ between patients. As a result, hypothesis tests comparing all patients to all healthy controls can detect many significant variables with inconsequential effect sizes. A few highly predictive root causes may nevertheless generate disease within each patient. In this paper, we define patient-specific root causes as variables subject to exogenous "shocks" which go on to perturb an otherwise healthy system and induce disease. In other words, the variables are associated with the exogenous errors of a structural equation model (SEM), and these errors predict a downstream diagnostic label. We quantify predictivity using sample-specific Shapley values. This derivation allows us to develop a fast algorithm called Root Causal Inference for identifying patient-specific root causes by extracting the error terms of a linear SEM and then computing the Shapley value associated with each error. Experiments highlight considerable improvements in accuracy because the method uncovers root causes that may have large effect sizes at the individual level but clinically insignificant effect sizes at the group level. An R implementation is available at github.com/ericstrobl/RCI.
Generalizing Clinical Trials with Convex Hulls
Nov 25, 2021

Randomized clinical trials eliminate confounding but impose strict exclusion criteria that limit recruitment to a subset of the population. Observational datasets are more inclusive but suffer from confounding -- often providing overly optimistic estimates of treatment effect in practice. We therefore assume that the true treatment effect lies somewhere in between no treatment effect and the observational estimate, or in their convex hull. This assumption allows us to extrapolate results from exclusive trials to the broader population by analyzing observational and trial data simultaneously using an algorithm called Optimal Convex Hulls (OCH). OCH represents the treatment effect either in terms of convex hulls of conditional expectations or convex hulls (also known as mixtures) of conditional densities. The algorithm first learns the component expectations or densities using the observational data and then learns the linear mixing coefficients using trial data in order to approximate the true treatment effect; theory importantly explains why this linear combination should hold. OCH estimates the treatment effect in terms both expectations and densities with state of the art accuracy.