 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeRigid Motion Estimation using Accelerated Iterative Coordinate Descent (REACT) for MR Imaging
Mar 24, 2026Purpose: To develop a computationally viable autofocus method for estimating 3D rigid motion in MR imaging. Theory and Methods: The proposed method, REACT, assumes a piecewise-constant motion trajectory and estimates the rigid motion parameters of individual temporal segments by optimizing an image-quality metric. Coordinate descent is adopted to decompose the high-dimensional optimization problem into a series of subproblems, each updating the motion parameters of a single temporal segment. The cost function of each subproblem is assumed to be approximately locally convex under suitable acquisition conditions. Each subproblem is then solved using a derivative-free solver, thereby avoiding an exhaustive grid search. Numerical simulations were conducted to investigate the local convexity assumption. REACT was evaluated for respiratory motion correction on in vivo free-breathing coronary MR angiography datasets acquired using a 3D cones trajectory with image-based navigators (iNAVs). An autofocus nonrigid motion correction method was also evaluated for comparison. Coronary artery sharpness was quantified using unbounded image edge profile acutance (u-IEPA). Results: In numerical simulations, the objective surfaces of the subproblems were approximately locally convex when the current motion estimate was close to the desired solution. In the in vivo study, REACT yielded higher u-IEPA than the conventional iNAV-based translational motion-estimation method for both the left anterior descending artery (LAD) and right coronary artery. REACT also yielded higher u-IEPA for the LAD than the autofocus nonrigid motion correction method. Conclusion: This study demonstrates the feasibility of coordinate descent for autofocus motion correction in MR imaging.
Image-Space Gridding for Nonrigid Motion-Corrected MR Image Reconstruction
Jan 28, 2025Motion remains a major challenge in magnetic resonance (MR) imaging, particularly in free-breathing cardiac MR imaging, where data are acquired over multiple heartbeats at varying respiratory phases. We adopt a model-based approach for nonrigid motion correction, addressing two challenges: (a) motion representation and (b) motion estimation. For motion representation, we derive image-space gridding by adapting the nonuniform fast Fourier transform (NUFFT) to represent and compute nonrigid motion, which provides an exact forward-adjoint pair of linear operators. We then introduce nonrigid SENSE operators that incorporate nonrigid motion into the multi-coil MR acquisition model. For motion estimation, we employ both low-resolution 3D image-based navigators (iNAVs) and high-resolution 3D self-navigating image-based navigators (self-iNAVs). During each heartbeat, data are acquired along two types of non-Cartesian trajectories: a subset of a high-resolution trajectory that sparsely covers 3D k-space, followed by a full low-resolution trajectory. We reconstruct 3D iNAVs for each heartbeat using the full low-resolution data, which are then used to estimate bulk motion and identify the respiratory phase of each heartbeat. By combining data from multiple heartbeats within the same respiratory phase, we reconstruct high-resolution 3D self-iNAVs, allowing estimation of nonrigid respiratory motion. For each respiratory phase, we construct the nonrigid SENSE operator, reformulating the nonrigid motion-corrected reconstruction as a standard regularized inverse problem. In a preliminary study, the proposed method enhanced sharpness of the coronary arteries and improved image quality in non-cardiac regions, outperforming translational motion-corrected reconstruction.
Anisotropic field-of-views in radial imaging
Jan 12, 2021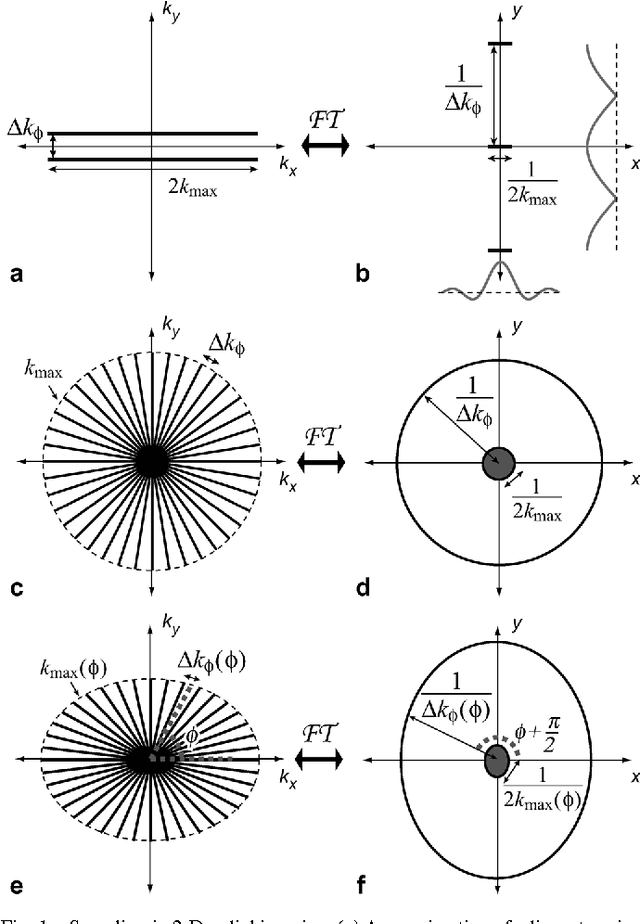
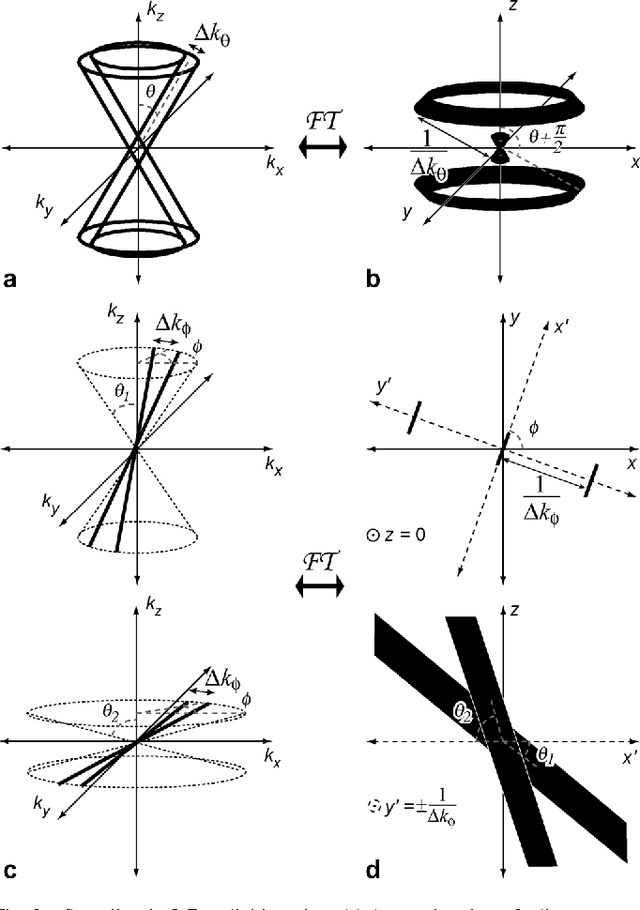
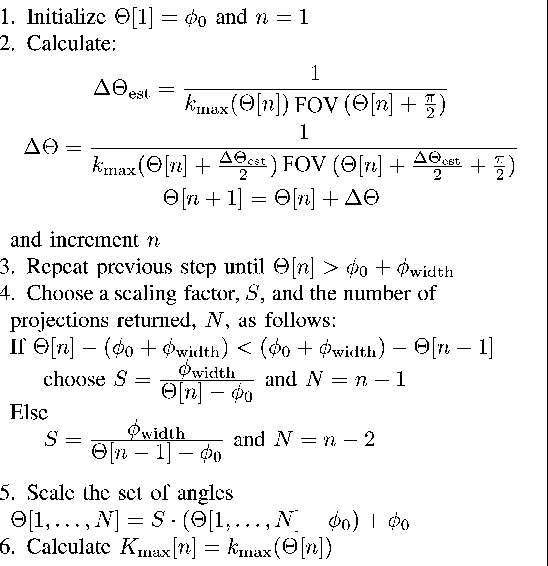

Radial imaging techniques, such as projection-reconstruction (PR), are used in magnetic resonance imaging (MRI) for dynamic imaging, angiography, and short-imaging. They are robust to flow and motion, have diffuse aliasing patterns, and support short readouts and echo times. One drawback is that standard implementations do not support anisotropic field-of-view (FOV) shapes, which are used to match the imaging parameters to the object or region-of-interest. A set of fast, simple algorithms for 2-D and 3-D PR, and 3-D cones acquisitions are introduced that match the sampling density in frequency space to the desired FOV shape. Tailoring the acquisitions allows for reduction of aliasing artifacts in undersampled applications or scan time reductions without introducing aliasing in fully-sampled applications. It also makes possible new radial imaging applications that were previously unsuitable, such as imaging elongated regions or thin slabs. 2-D PR longitudinal leg images and thin-slab, single breath-hold 3-D PR abdomen images, both with isotropic resolution, demonstrate these new possibilities. No scan time to volume efficiency is lost by using anisotropic FOVs. The acquisition trajectories can be computed on a scan by scan basis.
Reconstruction of Undersampled 3D Non-Cartesian Image-Based Navigators for Coronary MRA Using an Unrolled Deep Learning Model
Oct 24, 2019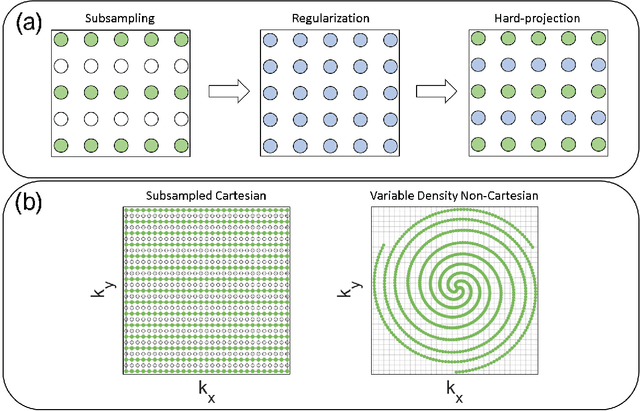

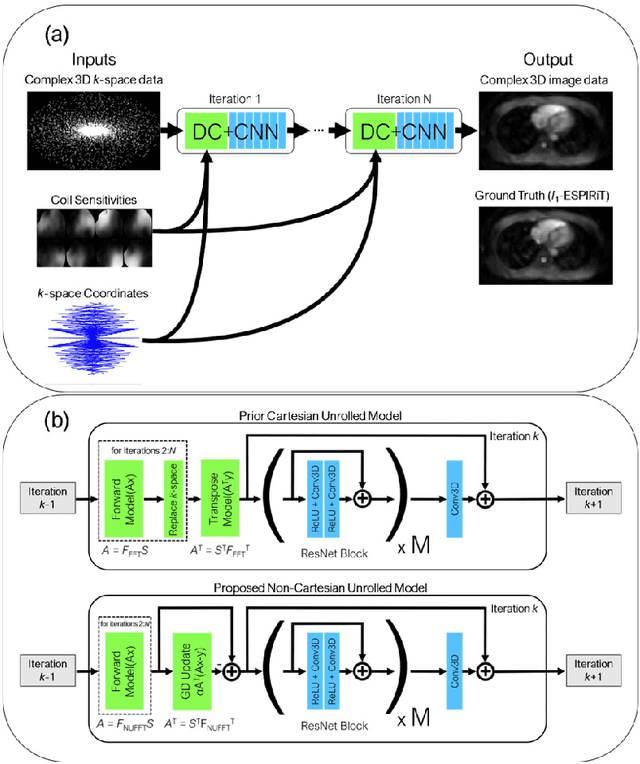
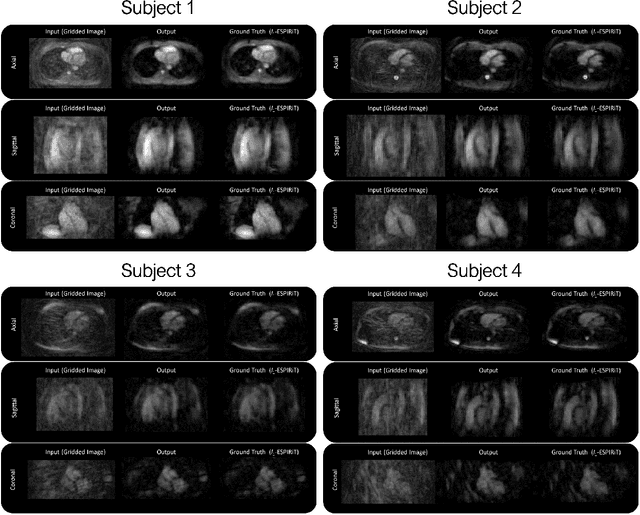
Purpose: To rapidly reconstruct undersampled 3D non-Cartesian image-based navigators (iNAVs) using an unrolled deep learning (DL) model for non-rigid motion correction in coronary magnetic resonance angiography (CMRA). Methods: An unrolled network is trained to reconstruct beat-to-beat 3D iNAVs acquired as part of a CMRA sequence. The unrolled model incorporates a non-uniform FFT operator to perform the data consistency operation, and the regularization term is learned by a convolutional neural network (CNN) based on the proximal gradient descent algorithm. The training set includes 6,000 3D iNAVs acquired from 7 different subjects and 11 scans using a variable-density (VD) cones trajectory. For testing, 3D iNAVs from 4 additional subjects are reconstructed using the unrolled model. To validate reconstruction accuracy, global and localized motion estimates from DL model-based 3D iNAVs are compared with those extracted from 3D iNAVs reconstructed with $\textit{l}_{1}$-ESPIRiT. Then, the high-resolution coronary MRA images motion corrected with autofocusing using the $\textit{l}_{1}$-ESPIRiT and DL model-based 3D iNAVs are assessed for differences. Results: 3D iNAVs reconstructed using the DL model-based approach and conventional $\textit{l}_{1}$-ESPIRiT generate similar global and localized motion estimates and provide equivalent coronary image quality. Reconstruction with the unrolled network completes in a fraction of the time compared to CPU and GPU implementations of $\textit{l}_{1}$-ESPIRiT (20x and 3x speed increases, respectively). Conclusion: We have developed a deep neural network architecture to reconstruct undersampled 3D non-Cartesian VD cones iNAVs. Our approach decreases reconstruction time for 3D iNAVs, while preserving the accuracy of non-rigid motion information offered by them for correction.