 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgePrompting Medical Large Vision-Language Models to Diagnose Pathologies by Visual Question Answering
Jul 31, 2024Large Vision-Language Models (LVLMs) have achieved significant success in recent years, and they have been extended to the medical domain. Although demonstrating satisfactory performance on medical Visual Question Answering (VQA) tasks, Medical LVLMs (MLVLMs) suffer from the hallucination problem, which makes them fail to diagnose complex pathologies. Moreover, they readily fail to learn minority pathologies due to imbalanced training data. We propose two prompting strategies for MLVLMs that reduce hallucination and improve VQA performance. In the first strategy, we provide a detailed explanation of the queried pathology. In the second strategy, we fine-tune a cheap, weak learner to achieve high performance on a specific metric, and textually provide its judgment to the MLVLM. Tested on the MIMIC-CXR-JPG and Chexpert datasets, our methods significantly improve the diagnostic F1 score, with the highest increase being 0.27. We also demonstrate that our prompting strategies can be extended to general LVLM domains. Based on POPE metrics, it effectively suppresses the false negative predictions of existing LVLMs and improves Recall by approximately 0.07.
A Mobility-Aware Deep Learning Model for Long-Term COVID-19 Pandemic Prediction and Policy Impact Analysis
Dec 05, 2022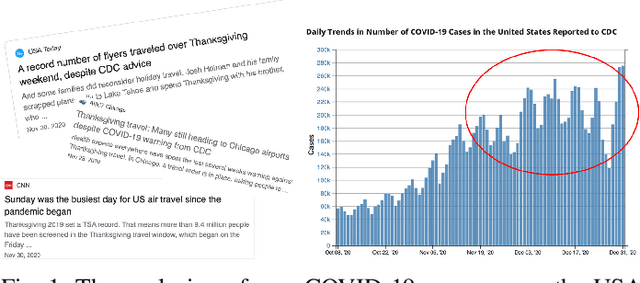
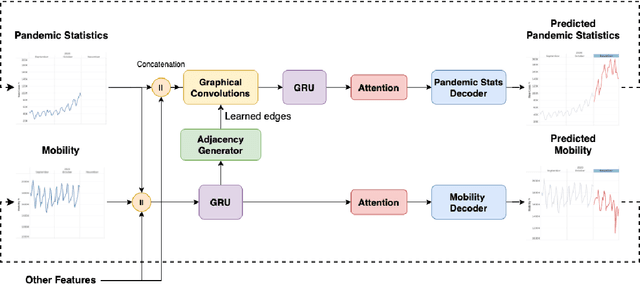
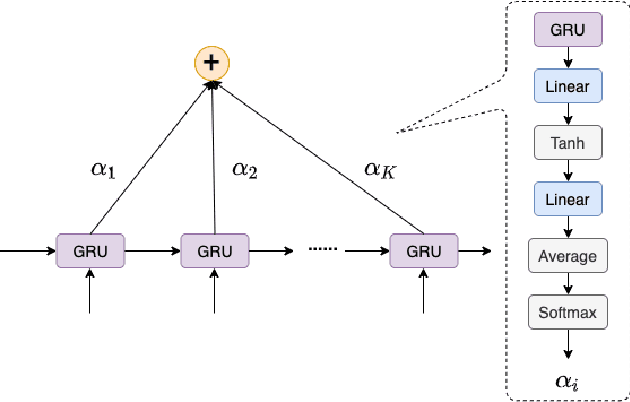
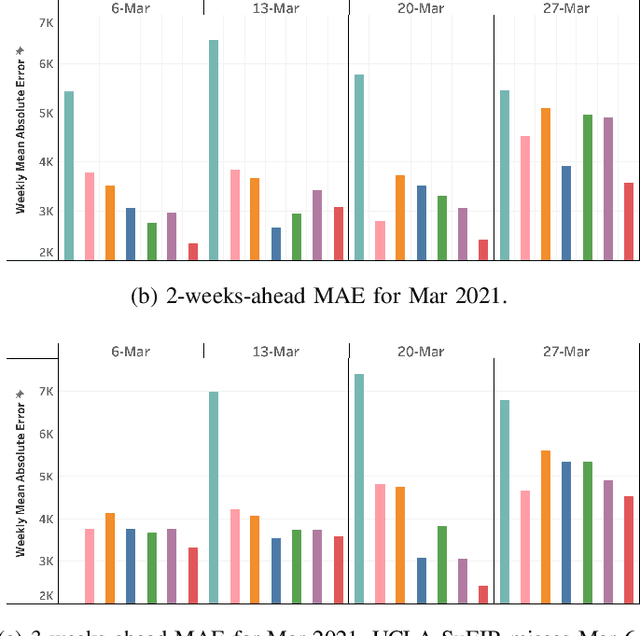
Pandemic(epidemic) modeling, aiming at disease spreading analysis, has always been a popular research topic especially following the outbreak of COVID-19 in 2019. Some representative models including SIR-based deep learning prediction models have shown satisfactory performance. However, one major drawback for them is that they fall short in their long-term predictive ability. Although graph convolutional networks (GCN) also perform well, their edge representations do not contain complete information and it can lead to biases. Another drawback is that they usually use input features which they are unable to predict. Hence, those models are unable to predict further future. We propose a model that can propagate predictions further into the future and it has better edge representations. In particular, we model the pandemic as a spatial-temporal graph whose edges represent the transition of infections and are learned by our model. We use a two-stream framework that contains GCN and recursive structures (GRU) with an attention mechanism. Our model enables mobility analysis that provides an effective toolbox for public health researchers and policy makers to predict how different lock-down strategies that actively control mobility can influence the spread of pandemics. Experiments show that our model outperforms others in its long-term predictive power. Moreover, we simulate the effects of certain policies and predict their impacts on infection control.