 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeCLIP Is Shortsighted: Paying Attention Beyond the First Sentence
Feb 25, 2026CLIP models learn transferable multi-modal features via image-text contrastive learning on internet-scale data. They are widely used in zero-shot classification, multi-modal retrieval, text-to-image diffusion, and as image encoders in large vision-language models. However, CLIP's pretraining is dominated by images paired with short captions, biasing the model toward encoding simple descriptions of salient objects and leading to coarse alignment on complex scenes and dense descriptions. While recent work mitigates this by fine-tuning on small-scale long-caption datasets, we identify an important common bias: both human- and LLM-generated long captions typically begin with a one-sentence summary followed by a detailed description. We show that this acts as a shortcut during training, concentrating attention on the opening sentence and early tokens and weakening alignment over the rest of the caption. To resolve this, we introduce DeBias-CLIP, which removes the summary sentence during training and applies sentence sub-sampling and text token padding to distribute supervision across all token positions. DeBias-CLIP achieves state-of-the-art long-text retrieval, improves short-text retrieval, and is less sensitive to sentence order permutations. It is a drop-in replacement for Long-CLIP with no additional trainable parameters.
Judging by the Rules: Compliance-Aligned Framework for Modern Slavery Statement Monitoring
Nov 11, 2025Modern slavery affects millions of people worldwide, and regulatory frameworks such as Modern Slavery Acts now require companies to publish detailed disclosures. However, these statements are often vague and inconsistent, making manual review time-consuming and difficult to scale. While NLP offers a promising path forward, high-stakes compliance tasks require more than accurate classification: they demand transparent, rule-aligned outputs that legal experts can verify. Existing applications of large language models (LLMs) often reduce complex regulatory assessments to binary decisions, lacking the necessary structure for robust legal scrutiny. We argue that compliance verification is fundamentally a rule-matching problem: it requires evaluating whether textual statements adhere to well-defined regulatory rules. To this end, we propose a novel framework that harnesses AI for rule-level compliance verification while preserving expert oversight. At its core is the Compliance Alignment Judge (CA-Judge), which evaluates model-generated justifications based on their fidelity to statutory requirements. Using this feedback, we train the Compliance Alignment LLM (CALLM), a model that produces rule-consistent, human-verifiable outputs. CALLM improves predictive performance and generates outputs that are both transparent and legally grounded, offering a more verifiable and actionable solution for real-world compliance analysis.
Towards Trustworthy Automatic Diagnosis Systems by Emulating Doctors' Reasoning with Deep Reinforcement Learning
Oct 13, 2022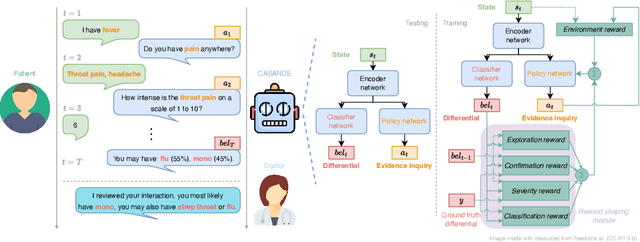
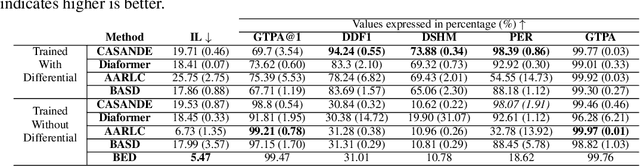
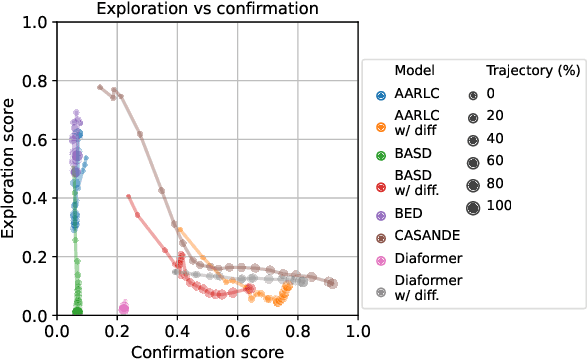
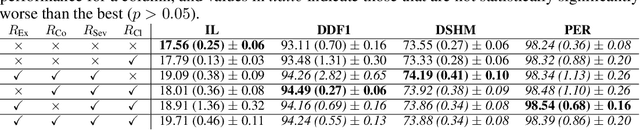
The automation of the medical evidence acquisition and diagnosis process has recently attracted increasing attention in order to reduce the workload of doctors and democratize access to medical care. However, most works proposed in the machine learning literature focus solely on improving the prediction accuracy of a patient's pathology. We argue that this objective is insufficient to ensure doctors' acceptability of such systems. In their initial interaction with patients, doctors do not only focus on identifying the pathology a patient is suffering from; they instead generate a differential diagnosis (in the form of a short list of plausible diseases) because the medical evidence collected from patients is often insufficient to establish a final diagnosis. Moreover, doctors explicitly explore severe pathologies before potentially ruling them out from the differential, especially in acute care settings. Finally, for doctors to trust a system's recommendations, they need to understand how the gathered evidences led to the predicted diseases. In particular, interactions between a system and a patient need to emulate the reasoning of doctors. We therefore propose to model the evidence acquisition and automatic diagnosis tasks using a deep reinforcement learning framework that considers three essential aspects of a doctor's reasoning, namely generating a differential diagnosis using an exploration-confirmation approach while prioritizing severe pathologies. We propose metrics for evaluating interaction quality based on these three aspects. We show that our approach performs better than existing models while maintaining competitive pathology prediction accuracy.
DDXPlus: A new Dataset for Medical Automatic Diagnosis
May 18, 2022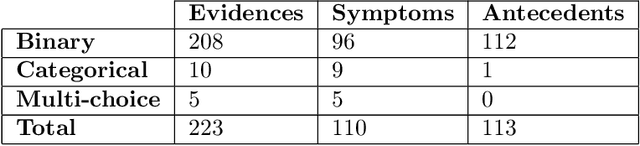
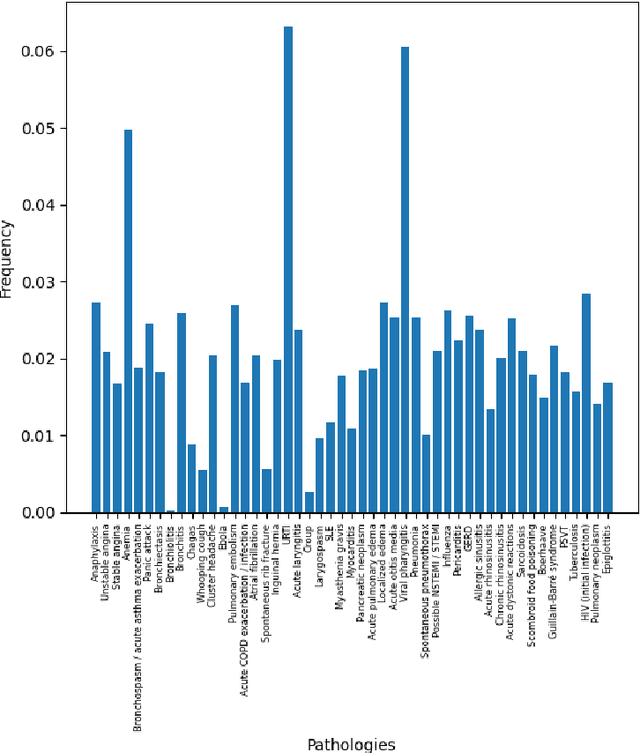
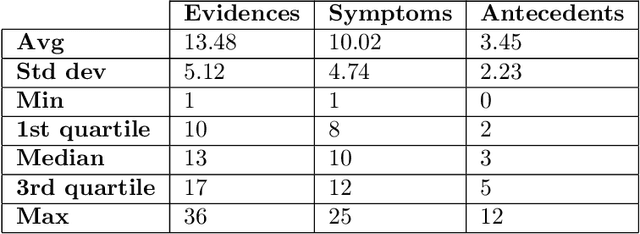
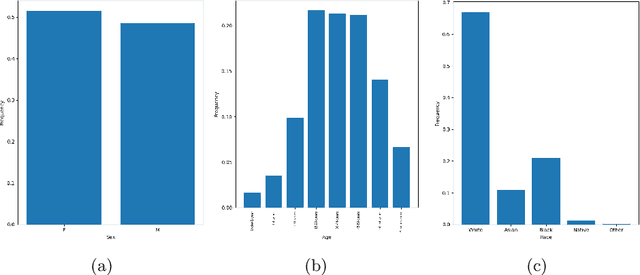
There has been rapidly growing interests in Automatic Diagnosis (AD) and Automatic Symptom Detection (ASD) systems in the machine learning research literature, aiming to assist doctors in telemedicine services. These systems are designed to interact with patients, collect evidence relevant to their concerns, and make predictions about the underlying diseases. Doctors would review the interaction, including the evidence and the predictions, before making their final decisions. Despite the recent progress, an important piece of doctors' interactions with patients is missing in the design of AD and ASD systems, namely the differential diagnosis. Its absence is largely due to the lack of datasets that include such information for models to train on. In this work, we present a large-scale synthetic dataset that includes a differential diagnosis, along with the ground truth pathology, for each patient. In addition, this dataset includes more pathologies, as well as types of symtoms and antecedents. As a proof-of-concept, we extend several existing AD and ASD systems to incorporate differential diagnosis, and provide empirical evidence that using differentials in training signals is essential for such systems to learn to predict differentials. Dataset available at https://github.com/bruzwen/ddxplus