 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeDiscovery of temporal structure intricacy in arterial blood pressure waveforms representing acuity of liver transplant and forecasting short term surgical outcome via unsupervised manifold learning
Sep 21, 2021



Background: Arterial blood pressure (ABP) waveform evolves across each consecutive pulse during the liver transplant surgery. We hypothesized that the quantification of the waveform evolution reflects 1) the acuity of the recipient undergoing liver transplant and 2) the intraoperative dynamics that forecasts short-term surgical outcomes. Methods: In this prospective observational single cohort study on living donor liver transplant surgery, we extracted the waveform morphological evolution from the ABP data with the unsupervised manifold learning waveform analysis. Two quantitative indices, trend movement and fluctuation movement, were developed to represent the slow-varying and fast-varying dynamics respectively. We investigated the associations with the liver disease acuity represented with the Model for End-Stage Liver Disease (MELD) score and the primary outcomes, the early allograft failure (EAF), as well as the recently developed EAF scores, including the Liver Graft Assessment Following Transplantation (L-GrAFT) score, the Early Allograft Failure Simplified Estimation (EASE) score, and the Model for Early Allograft Function (MEAF) score. Results: Sixty recipients were enrolled. The presurgical trend movement was correlated with the MELD scores. It decreased in the anhepatic phase. The neohepatic trend movement correlated with the L-GrAFT scores, the EASE score, and the MEAF score. Regarding the constituent of the EAF scores, the trend movement most correlated with the postoperative day 7 bilirubin. Conclusions: The ABP waveform evolution intricacy in the presurgical phase reflects recipients' acuity condition while that in the neohepatic phase reveal the short-term surgical outcome calculated from laboratory data in postoperative day 7-10. The waveform evolution reflects the intraoperative contribution to the early outcome.
Calibration for massive physiological signal collection in hospital -- Sawtooth artifact in beat-to-beat pulse transit time measured from patient monitor data
Aug 27, 2018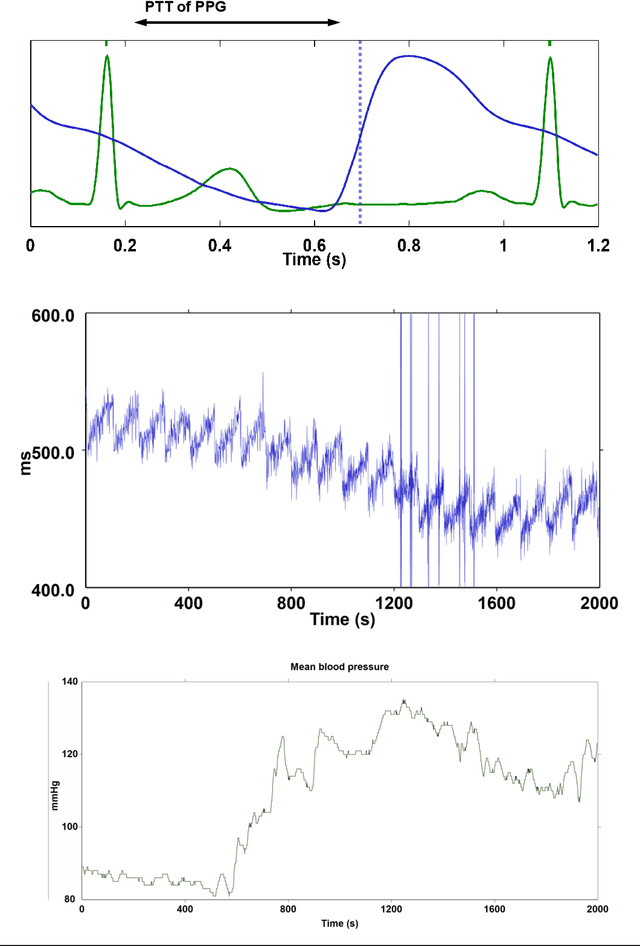
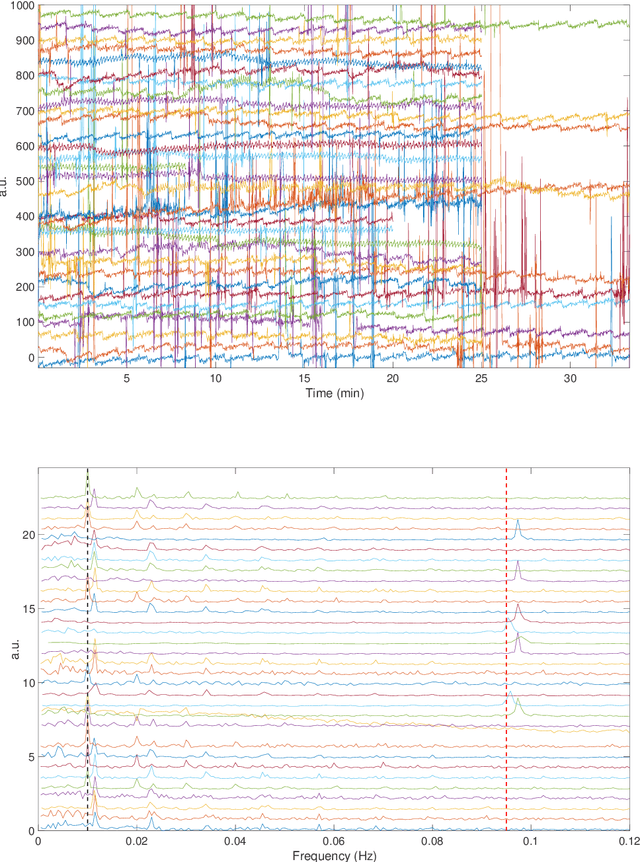


Objective: Calibration is one of the most important initial steps in any signal acquisition and experiment. It is however less discussed when massively collecting physiological signals in clinical setting. Here we test an off-the-shelf integrated Photoplethysmography (PPG) and electrocardiogram (ECG) monitoring device for its ability to yield a stable Pulse transit time (PTT) signal. Method: This is a retrospective clinical study using two databases: one containing 35 subjects who underwent laparoscopic cholecystectomy, another containing 22 subjects who underwent spontaneous breathing test in the intensive care unit. All data sets include recordings of PPG and ECG using a commonly deployed patient monitor. We calculated the PTT signal offline. Result: We identify a novel constant oscillatory pattern in the PTT signal and identify this pattern as the sawtooth artifact. We propose an approach based on the de-shape method to visualize, quantify and validate this sawtooth artifact. Conclusion: The PTT and ECG signals not designed for the PTT evaluation may contain unwanted artifacts. The PTT signal should be calibrated before analysis to avoid erroneous interpretation of its physiological meaning.