 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeTowards a Transportable Causal Network Model Based on Observational Healthcare Data
Nov 20, 2023


Over the last decades, many prognostic models based on artificial intelligence techniques have been used to provide detailed predictions in healthcare. Unfortunately, the real-world observational data used to train and validate these models are almost always affected by biases that can strongly impact the outcomes validity: two examples are values missing not-at-random and selection bias. Addressing them is a key element in achieving transportability and in studying the causal relationships that are critical in clinical decision making, going beyond simpler statistical approaches based on probabilistic association. In this context, we propose a novel approach that combines selection diagrams, missingness graphs, causal discovery and prior knowledge into a single graphical model to estimate the cardiovascular risk of adolescent and young females who survived breast cancer. We learn this model from data comprising two different cohorts of patients. The resulting causal network model is validated by expert clinicians in terms of risk assessment, accuracy and explainability, and provides a prognostic model that outperforms competing machine learning methods.
Causal Discovery with Missing Data in a Multicentric Clinical Study
May 17, 2023

Causal inference for testing clinical hypotheses from observational data presents many difficulties because the underlying data-generating model and the associated causal graph are not usually available. Furthermore, observational data may contain missing values, which impact the recovery of the causal graph by causal discovery algorithms: a crucial issue often ignored in clinical studies. In this work, we use data from a multi-centric study on endometrial cancer to analyze the impact of different missingness mechanisms on the recovered causal graph. This is achieved by extending state-of-the-art causal discovery algorithms to exploit expert knowledge without sacrificing theoretical soundness. We validate the recovered graph with expert physicians, showing that our approach finds clinically-relevant solutions. Finally, we discuss the goodness of fit of our graph and its consistency from a clinical decision-making perspective using graphical separation to validate causal pathways.
Risk Assessment of Lymph Node Metastases in Endometrial Cancer Patients: A Causal Approach
May 17, 2023



Assessing the pre-operative risk of lymph node metastases in endometrial cancer patients is a complex and challenging task. In principle, machine learning and deep learning models are flexible and expressive enough to capture the dynamics of clinical risk assessment. However, in this setting we are limited to observational data with quality issues, missing values, small sample size and high dimensionality: we cannot reliably learn such models from limited observational data with these sources of bias. Instead, we choose to learn a causal Bayesian network to mitigate the issues above and to leverage the prior knowledge on endometrial cancer available from clinicians and physicians. We introduce a causal discovery algorithm for causal Bayesian networks based on bootstrap resampling, as opposed to the single imputation used in related works. Moreover, we include a context variable to evaluate whether selection bias results in learning spurious associations. Finally, we discuss the strengths and limitations of our findings in light of the presence of missing data that may be missing-not-at-random, which is common in real-world clinical settings.
Weighted Positive Binary Decision Diagrams for Exact Probabilistic Inference
Oct 18, 2016



Recent work on weighted model counting has been very successfully applied to the problem of probabilistic inference in Bayesian networks. The probability distribution is encoded into a Boolean normal form and compiled to a target language, in order to represent local structure expressed among conditional probabilities more efficiently. We show that further improvements are possible, by exploiting the knowledge that is lost during the encoding phase and incorporating it into a compiler inspired by Satisfiability Modulo Theories. Constraints among variables are used as a background theory, which allows us to optimize the Shannon decomposition. We propose a new language, called Weighted Positive Binary Decision Diagrams, that reduces the cost of probabilistic inference by using this decomposition variant to induce an arithmetic circuit of reduced size.
Checking the Quality of Clinical Guidelines using Automated Reasoning Tools
Jun 02, 2008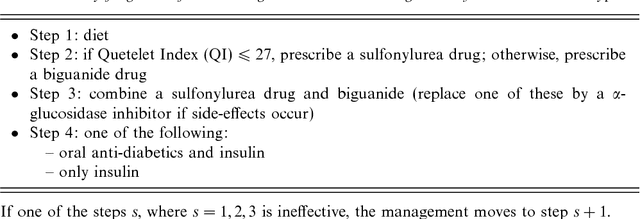
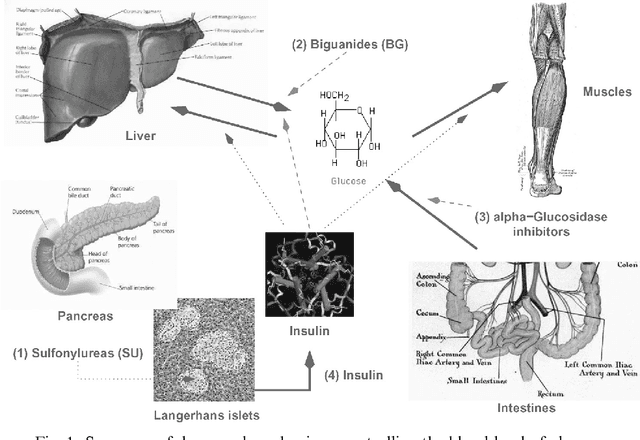


Requirements about the quality of clinical guidelines can be represented by schemata borrowed from the theory of abductive diagnosis, using temporal logic to model the time-oriented aspects expressed in a guideline. Previously, we have shown that these requirements can be verified using interactive theorem proving techniques. In this paper, we investigate how this approach can be mapped to the facilities of a resolution-based theorem prover, Otter, and a complementary program that searches for finite models of first-order statements, Mace. It is shown that the reasoning required for checking the quality of a guideline can be mapped to such fully automated theorem-proving facilities. The medical quality of an actual guideline concerning diabetes mellitus 2 is investigated in this way.