 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeDeepSOFA: A Continuous Acuity Score for Critically Ill Patients using Clinically Interpretable Deep Learning
Aug 30, 2018
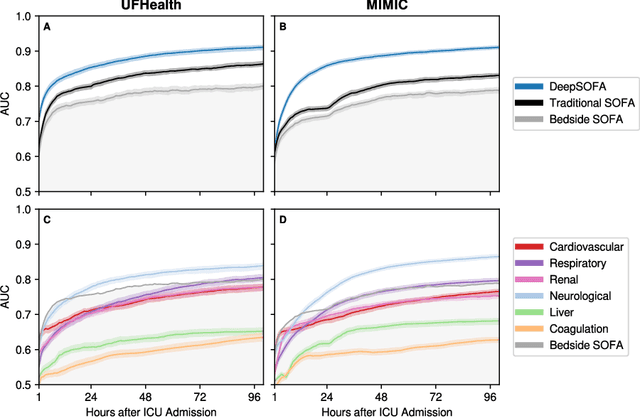
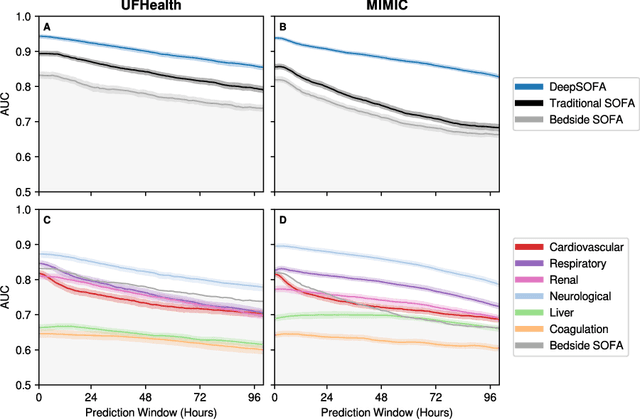
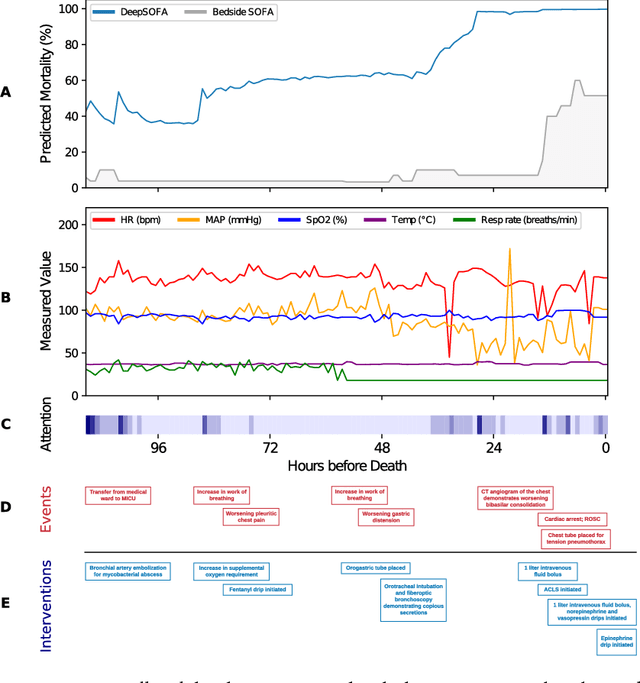
Traditional methods for assessing illness severity and predicting in-hospital mortality among critically ill patients require time-consuming, error-prone calculations using static variable thresholds. These methods do not capitalize on the emerging availability of streaming electronic health record data or capture time-sensitive individual physiological patterns, a critical task in the intensive care unit. We propose a novel acuity score framework (DeepSOFA) that leverages temporal measurements and interpretable deep learning models to assess illness severity at any point during an ICU stay. We compare DeepSOFA with SOFA (Sequential Organ Failure Assessment) baseline models using the same model inputs and find that at any point during an ICU admission, DeepSOFA yields significantly more accurate predictions of in-hospital mortality. A DeepSOFA model developed in a public database and validated in a single institutional cohort had a mean AUC for the entire ICU stay of 0.90 (95% CI 0.90-0.91) compared with baseline SOFA models with mean AUC 0.79 (95% CI 0.79-0.80) and 0.85 (95% CI 0.85-0.86). Deep models are well-suited to identify ICU patients in need of life-saving interventions prior to the occurrence of an unexpected adverse event and inform shared decision-making processes among patients, providers, and families regarding goals of care and optimal resource utilization.
Improved Predictive Models for Acute Kidney Injury with IDEAs: Intraoperative Data Embedded Analytics
May 11, 2018
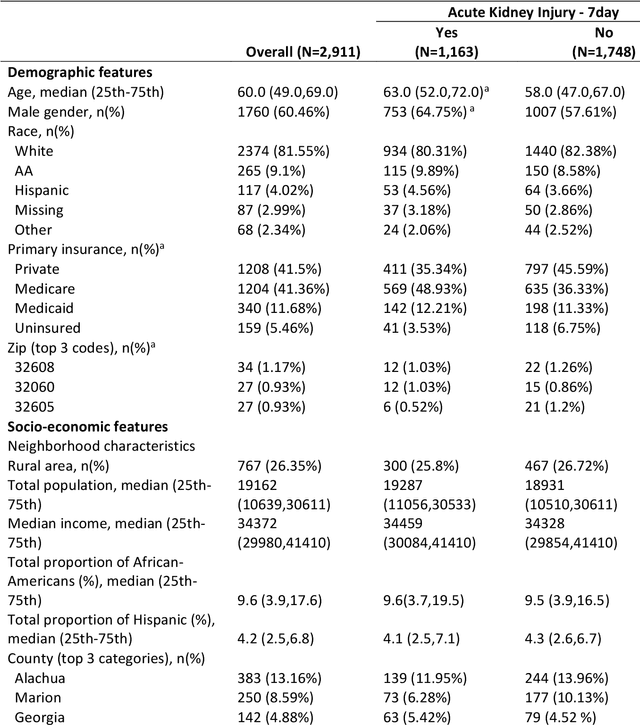

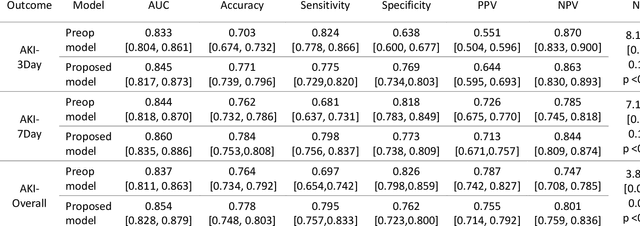
Acute kidney injury (AKI) is a common and serious complication after a surgery which is associated with morbidity and mortality. The majority of existing perioperative AKI risk score prediction models are limited in their generalizability and do not fully utilize the physiological intraoperative time-series data. Thus, there is a need for intelligent, accurate, and robust systems, able to leverage information from large-scale data to predict patient's risk of developing postoperative AKI. A retrospective single-center cohort of 2,911 adult patients who underwent surgery at the University of Florida Health has been used for this study. We used machine learning and statistical analysis techniques to develop perioperative models to predict the risk of AKI (risk during the first 3 days, 7 days, and until the discharge day) before and after the surgery. In particular, we examined the improvement in risk prediction by incorporating three intraoperative physiologic time series data, i.e., mean arterial blood pressure, minimum alveolar concentration, and heart rate. For an individual patient, the preoperative model produces a probabilistic AKI risk score, which will be enriched by integrating intraoperative statistical features through a machine learning stacking approach inside a random forest classifier. We compared the performance of our model based on the area under the receiver operating characteristics curve (AUROC), accuracy and net reclassification improvement (NRI). The predictive performance of the proposed model is better than the preoperative data only model. For AKI-7day outcome: The AUC was 0.86 (accuracy was 0.78) in the proposed model, while the preoperative AUC was 0.84 (accuracy 0.76). Furthermore, with the integration of intraoperative features, we were able to classify patients who were misclassified in the preoperative model.