 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeApproximate Bayesian Computation for an Explicit-Duration Hidden Markov Model of COVID-19 Hospital Trajectories
Apr 28, 2021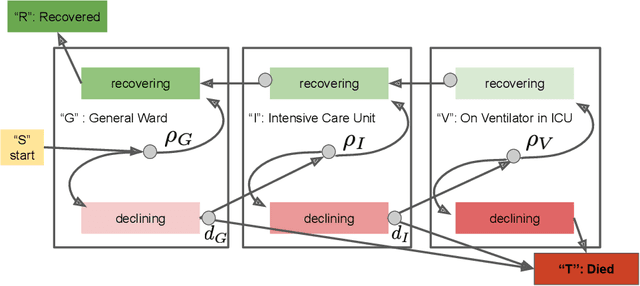
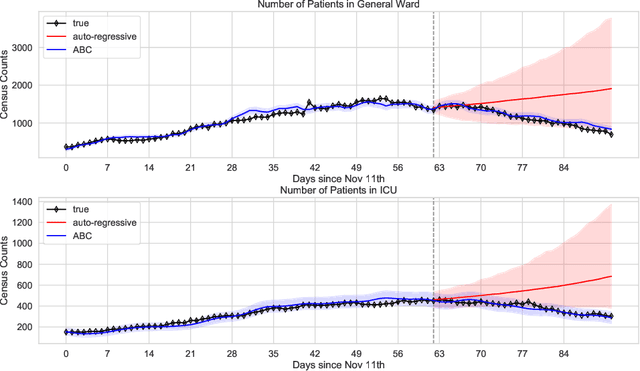
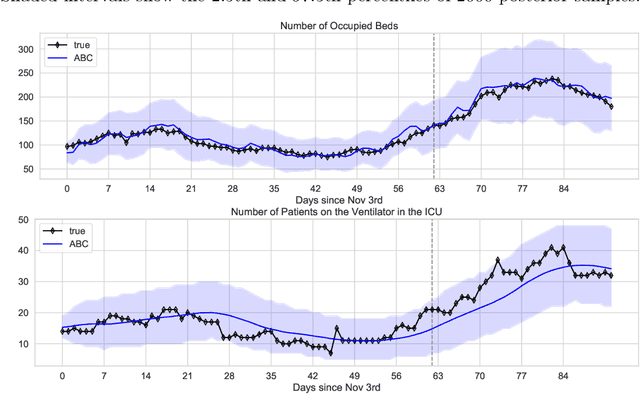
We address the problem of modeling constrained hospital resources in the midst of the COVID-19 pandemic in order to inform decision-makers of future demand and assess the societal value of possible interventions. For broad applicability, we focus on the common yet challenging scenario where patient-level data for a region of interest are not available. Instead, given daily admissions counts, we model aggregated counts of observed resource use, such as the number of patients in the general ward, in the intensive care unit, or on a ventilator. In order to explain how individual patient trajectories produce these counts, we propose an aggregate count explicit-duration hidden Markov model, nicknamed the ACED-HMM, with an interpretable, compact parameterization. We develop an Approximate Bayesian Computation approach that draws samples from the posterior distribution over the model's transition and duration parameters given aggregate counts from a specific location, thus adapting the model to a region or individual hospital site of interest. Samples from this posterior can then be used to produce future forecasts of any counts of interest. Using data from the United States and the United Kingdom, we show our mechanistic approach provides competitive probabilistic forecasts for the future even as the dynamics of the pandemic shift. Furthermore, we show how our model provides insight about recovery probabilities or length of stay distributions, and we suggest its potential to answer challenging what-if questions about the societal value of possible interventions.
Forecasting COVID-19 Counts At A Single Hospital: A Hierarchical Bayesian Approach
Apr 14, 2021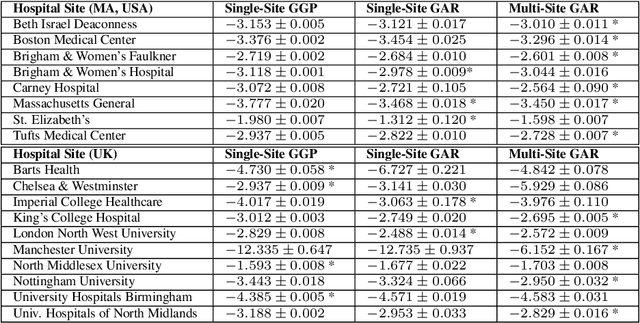
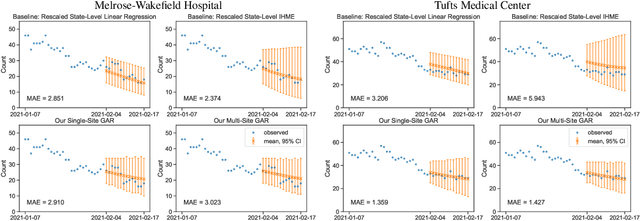
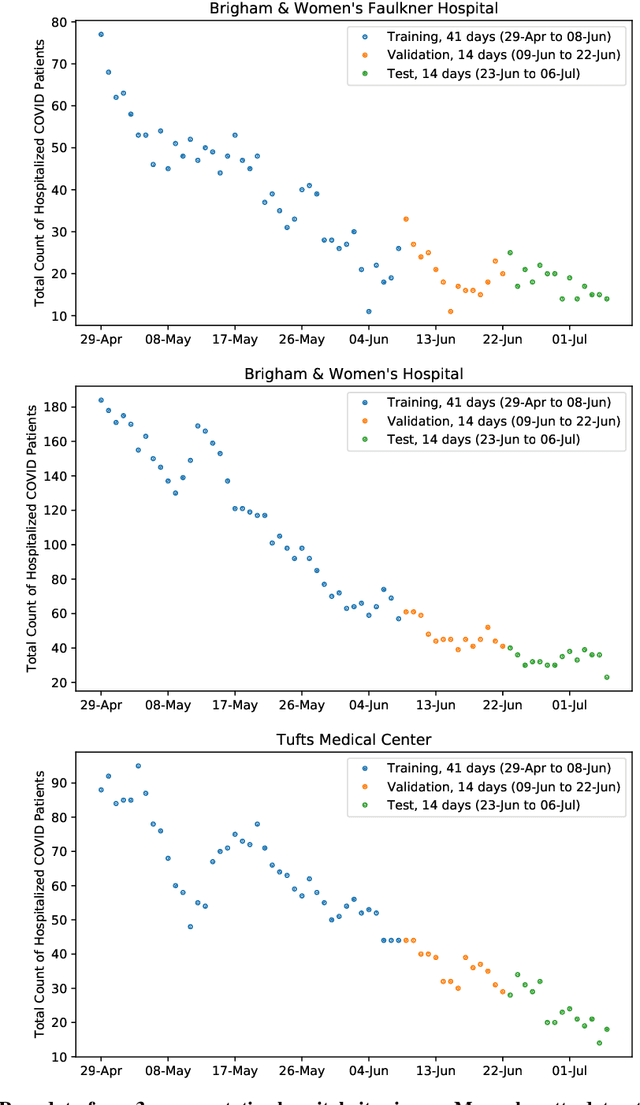
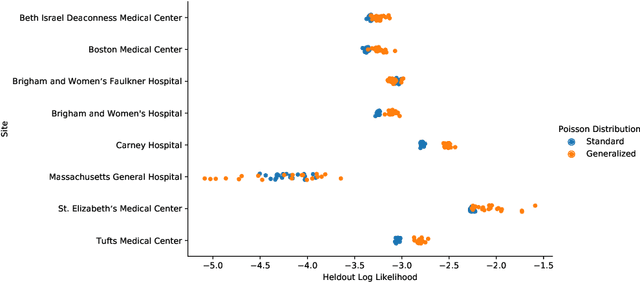
We consider the problem of forecasting the daily number of hospitalized COVID-19 patients at a single hospital site, in order to help administrators with logistics and planning. We develop several candidate hierarchical Bayesian models which directly capture the count nature of data via a generalized Poisson likelihood, model time-series dependencies via autoregressive and Gaussian process latent processes, and share statistical strength across related sites. We demonstrate our approach on public datasets for 8 hospitals in Massachusetts, U.S.A. and 10 hospitals in the United Kingdom. Further prospective evaluation compares our approach favorably to baselines currently used by stakeholders at 3 related hospitals to forecast 2-week-ahead demand by rescaling state-level forecasts.