 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeEnabling High-Curvature Navigation in Eversion Robots through Buckle-Inducing Constrictive Bands
Jan 18, 2026Tip-growing eversion robots are renowned for their ability to access remote spaces through narrow passages. However, achieving reliable navigation remains a significant challenge. Existing solutions often rely on artificial muscles integrated into the robot body or active tip-steering mechanisms. While effective, these additions introduce structural complexity and compromise the defining advantages of eversion robots: their inherent softness and compliance. In this paper, we propose a passive approach to reduce bending stiffness by purposefully introducing buckling points along the robot's outer wall. We achieve this by integrating inextensible diameter-reducing circumferential bands at regular intervals along the robot body facilitating forward motion through tortuous, obstacle cluttered paths. Rather than relying on active steering, our approach leverages the robot's natural interaction with the environment, allowing for smooth, compliant navigation. We present a Cosserat rod-based mathematical model to quantify this behavior, capturing the local stiffness reductions caused by the constricting bands and their impact on global bending mechanics. Experimental results demonstrate that these bands reduce the robot's stiffness when bent at the tip by up to 91 percent, enabling consistent traversal of 180 degree bends with a bending radius of as low as 25 mm-notably lower than the 35 mm achievable by standard eversion robots under identical conditions. The feasibility of the proposed method is further demonstrated through a case study in a colon phantom. By significantly improving maneuverability without sacrificing softness or increasing mechanical complexity, this approach expands the applicability of eversion robots in highly curved pathways, whether in relation to pipe inspection or medical procedures such as colonoscopy.
Reinforcement Learning for Safe Autonomous Two Device Navigation of Cerebral Vessels in Mechanical Thrombectomy
Mar 31, 2025Purpose: Autonomous systems in mechanical thrombectomy (MT) hold promise for reducing procedure times, minimizing radiation exposure, and enhancing patient safety. However, current reinforcement learning (RL) methods only reach the carotid arteries, are not generalizable to other patient vasculatures, and do not consider safety. We propose a safe dual-device RL algorithm that can navigate beyond the carotid arteries to cerebral vessels. Methods: We used the Simulation Open Framework Architecture to represent the intricacies of cerebral vessels, and a modified Soft Actor-Critic RL algorithm to learn, for the first time, the navigation of micro-catheters and micro-guidewires. We incorporate patient safety metrics into our reward function by integrating guidewire tip forces. Inverse RL is used with demonstrator data on 12 patient-specific vascular cases. Results: Our simulation demonstrates successful autonomous navigation within unseen cerebral vessels, achieving a 96% success rate, 7.0s procedure time, and 0.24 N mean forces, well below the proposed 1.5 N vessel rupture threshold. Conclusion: To the best of our knowledge, our proposed autonomous system for MT two-device navigation reaches cerebral vessels, considers safety, and is generalizable to unseen patient-specific cases for the first time. We envisage future work will extend the validation to vasculatures of different complexity and on in vitro models. While our contributions pave the way towards deploying agents in clinical settings, safety and trustworthiness will be crucial elements to consider when proposing new methodology.
Artificial Intelligence in the Autonomous Navigation of Endovascular Interventions: A Systematic Review
May 06, 2024
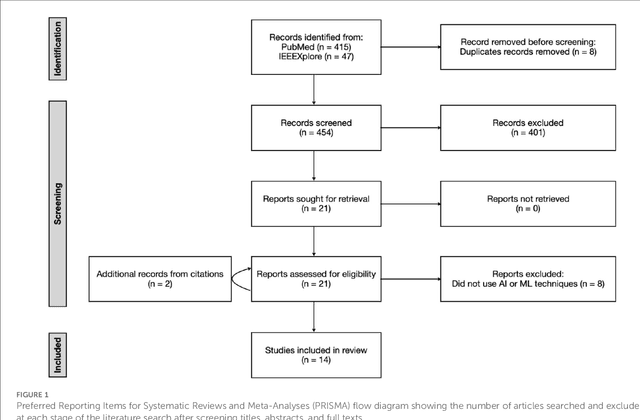

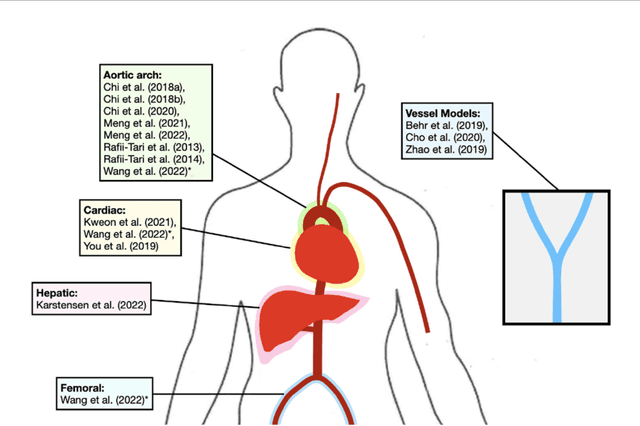
Purpose: Autonomous navigation of devices in endovascular interventions can decrease operation times, improve decision-making during surgery, and reduce operator radiation exposure while increasing access to treatment. This systematic review explores recent literature to assess the impact, challenges, and opportunities artificial intelligence (AI) has for the autonomous endovascular intervention navigation. Methods: PubMed and IEEEXplore databases were queried. Eligibility criteria included studies investigating the use of AI in enabling the autonomous navigation of catheters/guidewires in endovascular interventions. Following PRISMA, articles were assessed using QUADAS-2. PROSPERO: CRD42023392259. Results: Among 462 studies, fourteen met inclusion criteria. Reinforcement learning (9/14, 64%) and learning from demonstration (7/14, 50%) were used as data-driven models for autonomous navigation. Studies predominantly utilised physical phantoms (10/14, 71%) and in silico (4/14, 29%) models. Experiments within or around the blood vessels of the heart were reported by the majority of studies (10/14, 71%), while simple non-anatomical vessel platforms were used in three studies (3/14, 21%), and the porcine liver venous system in one study. We observed that risk of bias and poor generalisability were present across studies. No procedures were performed on patients in any of the studies reviewed. Studies lacked patient selection criteria, reference standards, and reproducibility, resulting in low clinical evidence levels. Conclusions: AI's potential in autonomous endovascular navigation is promising, but in an experimental proof-of-concept stage, with a technology readiness level of 3. We highlight that reference standards with well-identified performance metrics are crucial to allow for comparisons of data-driven algorithms proposed in the years to come.
* Abstract shortened for arXiv character limit