 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeReconsidering evaluation practices in modular systems: On the propagation of errors in MRI prostate cancer detection
Sep 15, 2023Magnetic resonance imaging has evolved as a key component for prostate cancer (PCa) detection, substantially increasing the radiologist workload. Artificial intelligence (AI) systems can support radiological assessment by segmenting and classifying lesions in clinically significant (csPCa) and non-clinically significant (ncsPCa). Commonly, AI systems for PCa detection involve an automatic prostate segmentation followed by the lesion detection using the extracted prostate. However, evaluation reports are typically presented in terms of detection under the assumption of the availability of a highly accurate segmentation and an idealistic scenario, omitting the propagation of errors between modules. For that purpose, we evaluate the effect of two different segmentation networks (s1 and s2) with heterogeneous performances in the detection stage and compare it with an idealistic setting (s1:89.90+-2.23 vs 88.97+-3.06 ncsPCa, P<.001, 89.30+-4.07 and 88.12+-2.71 csPCa, P<.001). Our results depict the relevance of a holistic evaluation, accounting for all the sub-modules involved in the system.
Leveraging multi-view data without annotations for prostate MRI segmentation: A contrastive approach
Aug 12, 2023

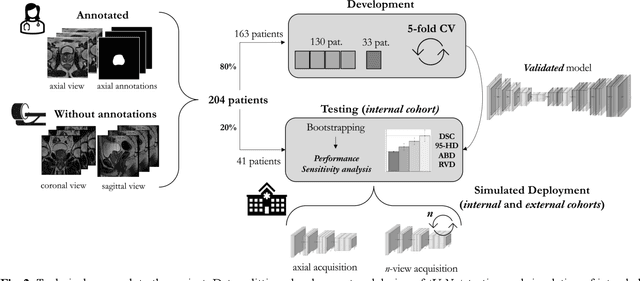

An accurate prostate delineation and volume characterization can support the clinical assessment of prostate cancer. A large amount of automatic prostate segmentation tools consider exclusively the axial MRI direction in spite of the availability as per acquisition protocols of multi-view data. Further, when multi-view data is exploited, manual annotations and availability at test time for all the views is commonly assumed. In this work, we explore a contrastive approach at training time to leverage multi-view data without annotations and provide flexibility at deployment time in the event of missing views. We propose a triplet encoder and single decoder network based on U-Net, tU-Net (triplet U-Net). Our proposed architecture is able to exploit non-annotated sagittal and coronal views via contrastive learning to improve the segmentation from a volumetric perspective. For that purpose, we introduce the concept of inter-view similarity in the latent space. To guide the training, we combine a dice score loss calculated with respect to the axial view and its manual annotations together with a multi-view contrastive loss. tU-Net shows statistical improvement in dice score coefficient (DSC) with respect to only axial view (91.25+-0.52% compared to 86.40+-1.50%,P<.001). Sensitivity analysis reveals the volumetric positive impact of the contrastive loss when paired with tU-Net (2.85+-1.34% compared to 3.81+-1.88%,P<.001). Further, our approach shows good external volumetric generalization in an in-house dataset when tested with multi-view data (2.76+-1.89% compared to 3.92+-3.31%,P=.002), showing the feasibility of exploiting non-annotated multi-view data through contrastive learning whilst providing flexibility at deployment in the event of missing views.
Prostate Age Gap : An MRI surrogate marker of aging for prostate cancer detection
Aug 10, 2023Background: Prostate cancer (PC) MRI-based risk calculators are commonly based on biological (e.g. PSA), MRI markers (e.g. volume), and patient age. Whilst patient age measures the amount of years an individual has existed, biological age (BA) might better reflect the physiology of an individual. However, surrogates from prostate MRI and linkage with clinically significant PC (csPC) remain to be explored. Purpose: To obtain and evaluate Prostate Age Gap (PAG) as an MRI marker tool for csPC risk. Study type: Retrospective. Population: A total of 7243 prostate MRI slices from 468 participants who had undergone prostate biopsies. A deep learning model was trained on 3223 MRI slices cropped around the gland from 81 low-grade PC (ncsPC, Gleason score <=6) and 131 negative cases and tested on the remaining 256 participants. Assessment: Chronological age was defined as the age of the participant at the time of the visit and used to train the deep learning model to predict the age of the patient. Following, we obtained PAG, defined as the model predicted age minus the patient's chronological age. Multivariate logistic regression models were used to estimate the association through odds ratio (OR) and predictive value of PAG and compared against PSA levels and PI-RADS>=3. Statistical tests: T-test, Mann-Whitney U test, Permutation test and ROC curve analysis. Results: The multivariate adjusted model showed a significant difference in the odds of clinically significant PC (csPC, Gleason score >=7) (OR =3.78, 95% confidence interval (CI):2.32-6.16, P <.001). PAG showed a better predictive ability when compared to PI-RADS>=3 and adjusted by other risk factors, including PSA levels: AUC =0.981 vs AUC =0.704, p<.001. Conclusion: PAG was significantly associated with the risk of clinically significant PC and outperformed other well-established PC risk factors.