 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeToward Accurate and Accessible Markerless Neuronavigation
Feb 04, 2026Neuronavigation is widely used in biomedical research and interventions to guide the precise placement of instruments around the head to support procedures such as transcranial magnetic stimulation. Traditional systems, however, rely on subject-mounted markers that require manual registration, may shift during procedures, and can cause discomfort. We introduce and evaluate markerless approaches that replace expensive hardware and physical markers with low-cost visible and infrared light cameras incorporating stereo and depth sensing combined with algorithmic modeling of the facial geometry. Validation with $50$ human subjects yielded a median tracking discrepancy of only $2.32$ mm and $2.01°$ for the best markerless algorithms compared to a conventional marker-based system, which indicates sufficient accuracy for transcranial magnetic stimulation and a substantial improvement over prior markerless results. The results suggest that integration of the data from the various camera sensors can improve the overall accuracy further. The proposed markerless neuronavigation methods can reduce setup cost and complexity, improve patient comfort, and expand access to neuronavigation in clinical and research settings.
Offline Learning of Closed-Loop Deep Brain Stimulation Controllers for Parkinson Disease Treatment
Feb 09, 2023


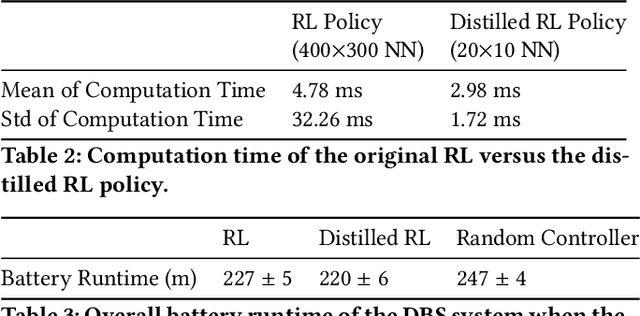
Deep brain stimulation (DBS) has shown great promise toward treating motor symptoms caused by Parkinson's disease (PD), by delivering electrical pulses to the Basal Ganglia (BG) region of the brain. However, DBS devices approved by the U.S. Food and Drug Administration (FDA) can only deliver continuous DBS (cDBS) stimuli at a fixed amplitude; this energy inefficient operation reduces battery lifetime of the device, cannot adapt treatment dynamically for activity, and may cause significant side-effects (e.g., gait impairment). In this work, we introduce an offline reinforcement learning (RL) framework, allowing the use of past clinical data to train an RL policy to adjust the stimulation amplitude in real time, with the goal of reducing energy use while maintaining the same level of treatment (i.e., control) efficacy as cDBS. Moreover, clinical protocols require the safety and performance of such RL controllers to be demonstrated ahead of deployments in patients. Thus, we also introduce an offline policy evaluation (OPE) method to estimate the performance of RL policies using historical data, before deploying them on patients. We evaluated our framework on four PD patients equipped with the RC+S DBS system, employing the RL controllers during monthly clinical visits, with the overall control efficacy evaluated by severity of symptoms (i.e., bradykinesia and tremor), changes in PD biomakers (i.e., local field potentials), and patient ratings. The results from clinical experiments show that our RL-based controller maintains the same level of control efficacy as cDBS, but with significantly reduced stimulation energy. Further, the OPE method is shown effective in accurately estimating and ranking the expected returns of RL controllers.