 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeOptimizing Medical Treatment for Sepsis in Intensive Care: from Reinforcement Learning to Pre-Trial Evaluation
Mar 18, 2020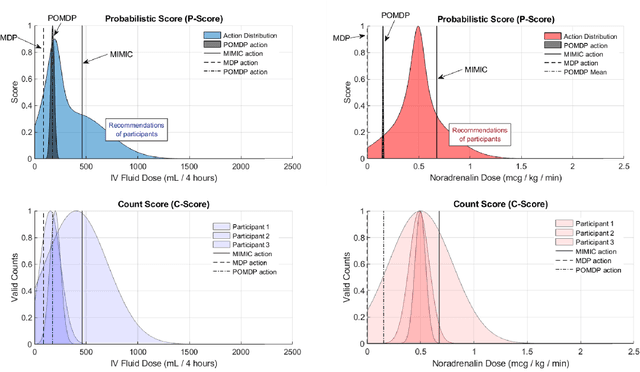
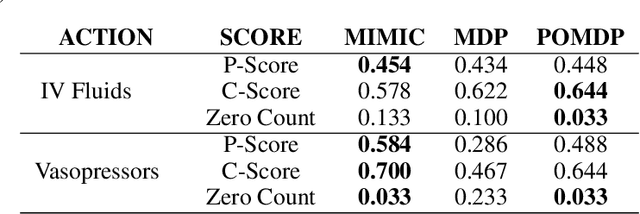
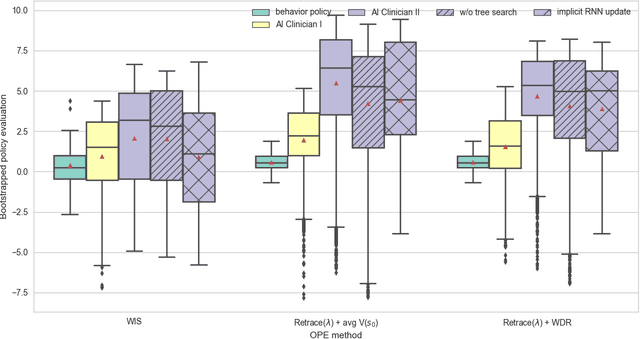
Our aim is to establish a framework where reinforcement learning (RL) of optimizing interventions retrospectively allows us a regulatory compliant pathway to prospective clinical testing of the learned policies in a clinical deployment. We focus on infections in intensive care units which are one of the major causes of death and difficult to treat because of the complex and opaque patient dynamics, and the clinically debated, highly-divergent set of intervention policies required by each individual patient, yet intensive care units are naturally data rich. In our work, we build on RL approaches in healthcare ("AI Clinicians"), and learn off-policy continuous dosing policy of pharmaceuticals for sepsis treatment using historical intensive care data under partially observable MDPs (POMDPs). POMPDs capture uncertainty in patient state better by taking in all historical information, yielding an efficient representation, which we investigate through ablations. We compensate for the lack of exploration in our retrospective data by evaluating each encountered state with a best-first tree search. We mitigate state distributional shift by optimizing our policy in the vicinity of the clinicians' compound policy. Crucially, we evaluate our model recommendations using not only conventional policy evaluations but a novel framework that incorporates human experts: a model-agnostic pre-clinical evaluation method to estimate the accuracy and uncertainty of clinician's decisions versus our system recommendations when confronted with the same individual patient history ("shadow mode").
Optimizing Sequential Medical Treatments with Auto-Encoding Heuristic Search in POMDPs
May 17, 2019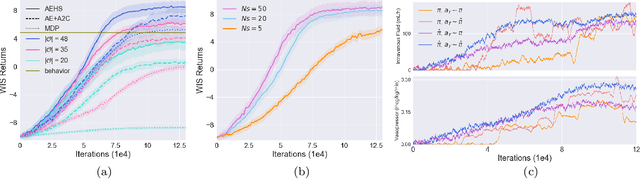
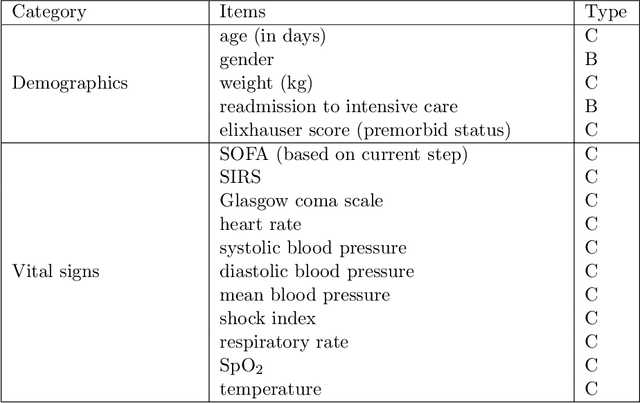
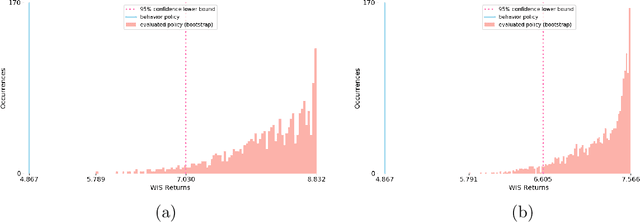
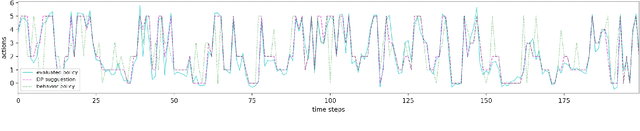
Health-related data is noisy and stochastic in implying the true physiological states of patients, limiting information contained in single-moment observations for sequential clinical decision making. We model patient-clinician interactions as partially observable Markov decision processes (POMDPs) and optimize sequential treatment based on belief states inferred from history sequence. To facilitate inference, we build a variational generative model and boost state representation with a recurrent neural network (RNN), incorporating an auxiliary loss from sequence auto-encoding. Meanwhile, we optimize a continuous policy of drug levels with an actor-critic method where policy gradients are obtained from a stablized off-policy estimate of advantage function, with the value of belief state backed up by parallel best-first suffix trees. We exploit our methodology in optimizing dosages of vasopressor and intravenous fluid for sepsis patients using a retrospective intensive care dataset and evaluate the learned policy with off-policy policy evaluation (OPPE). The results demonstrate that modelling as POMDPs yields better performance than MDPs, and that incorporating heuristic search improves sample efficiency.
The Actor Search Tree Critic for Off-Policy POMDP Learning in Medical Decision Making
Jun 03, 2018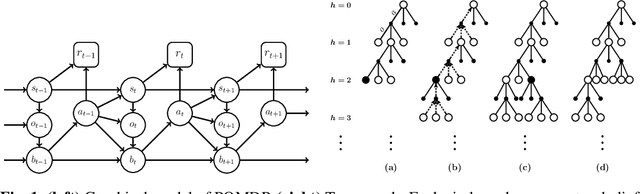
Off-policy reinforcement learning enables near-optimal policy from suboptimal experience, thereby provisions opportunity for artificial intelligence applications in healthcare. Previous works have mainly framed patient-clinician interactions as Markov decision processes, while true physiological states are not necessarily fully observable from clinical data. We capture this situation with partially observable Markov decision process, in which an agent optimises its actions in a belief represented as a distribution of patient states inferred from individual history trajectories. A Gaussian mixture model is fitted for the observed data. Moreover, we take into account the fact that nuance in pharmaceutical dosage could presumably result in significantly different effect by modelling a continuous policy through a Gaussian approximator directly in the policy space, i.e. the actor. To address the challenge of infinite number of possible belief states which renders exact value iteration intractable, we evaluate and plan for only every encountered belief, through heuristic search tree by tightly maintaining lower and upper bounds of the true value of belief. We further resort to function approximations to update value bounds estimation, i.e. the critic, so that the tree search can be improved through more compact bounds at the fringe nodes that will be back-propagated to the root. Both actor and critic parameters are learned via gradient-based approaches. Our proposed policy trained from real intensive care unit data is capable of dictating dosing on vasopressors and intravenous fluids for sepsis patients that lead to the best patient outcomes.