 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeDevelopment of Computable Phenotype to Identify and Characterize Transitions in Acuity Status in Intensive Care Unit
Apr 27, 2020
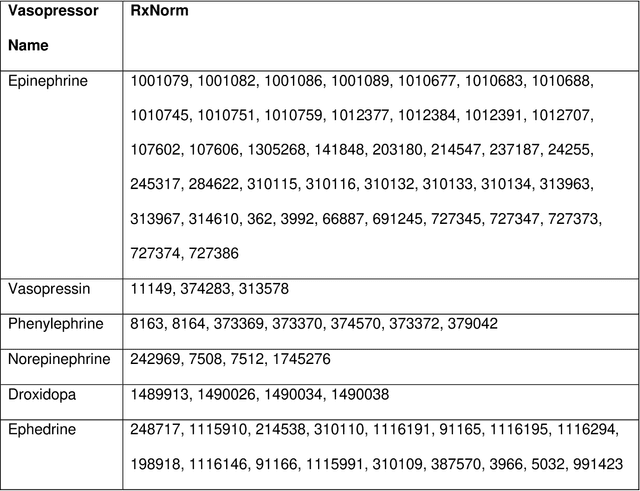
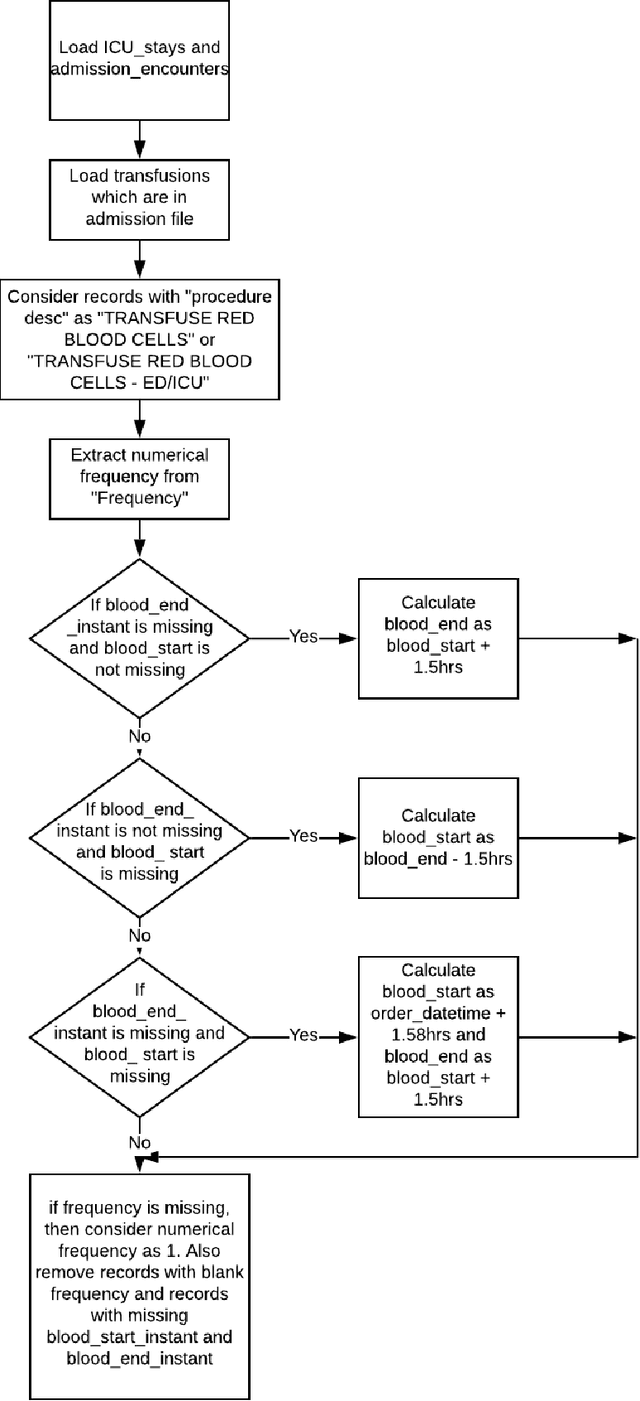

Background: In the United States, 5.7 million patients are admitted annually to intensive care units (ICU), with costs exceeding $82 billion. Although close monitoring and dynamic assessment of patient acuity are key aspects of ICU care, both are limited by the time constraints imposed on healthcare providers. Methods: Using the University of Florida Health (UFH) Integrated Data Repository as Honest Broker, we created a database with electronic health records data from a retrospective study cohort of 38,749 adult patients admitted to ICU at UF Health between 06/01/2014 and 08/22/2019. This repository includes demographic information, comorbidities, vital signs, laboratory values, medications with date and timestamps, and diagnoses and procedure codes for all index admission encounters as well as encounters within 12 months prior to index admission and 12 months follow-up. We developed algorithms to identify acuity status of the patient every four hours during each ICU stay. Results: We had 383,193 encounters (121,800 unique patients) admitted to the hospital, and 51,073 encounters (38,749 unique patients) with at least one ICU stay that lasted more than four hours. These patients requiring ICU admission had longer median hospital stay (7 days vs. 1 day) and higher in-hospital mortality (9.6% vs. 0.4%) compared with those not admitted to the ICU. Among patients who were admitted to the ICU and expired during hospital admission, more deaths occurred in the ICU than on general hospital wards (7.4% vs. 0.8%, respectively). Conclusions: We developed phenotyping algorithms that determined patient acuity status every four hours while admitted to the ICU. This approach may be useful in developing prognostic and clinical decision-support tools to aid patients, caregivers, and providers in shared decision-making processes regarding resource use and escalation of care.