 Add to Chrome
Add to Chrome Add to Firefox
Add to Firefox Add to Edge
Add to EdgeA Frame-based Attention Interpretation Method for Relevant Acoustic Feature Extraction in Long Speech Depression Detection
Jun 07, 2024


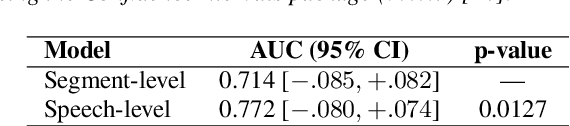
Speech-based depression detection tools could help early screening of depression. Here, we address two issues that may hinder the clinical practicality of such tools: segment-level labelling noise and a lack of model interpretability. We propose a speech-level Audio Spectrogram Transformer to avoid segment-level labelling. We observe that the proposed model significantly outperforms a segment-level model, providing evidence for the presence of segment-level labelling noise in audio modality and the advantage of longer-duration speech analysis for depression detection. We introduce a frame-based attention interpretation method to extract acoustic features from prediction-relevant waveform signals for interpretation by clinicians. Through interpretation, we observe that the proposed model identifies reduced loudness and F0 as relevant signals of depression, which aligns with the speech characteristics of depressed patients documented in clinical studies.
Hierarchical attention interpretation: an interpretable speech-level transformer for bi-modal depression detection
Sep 23, 2023Depression is a common mental disorder. Automatic depression detection tools using speech, enabled by machine learning, help early screening of depression. This paper addresses two limitations that may hinder the clinical implementations of such tools: noise resulting from segment-level labelling and a lack of model interpretability. We propose a bi-modal speech-level transformer to avoid segment-level labelling and introduce a hierarchical interpretation approach to provide both speech-level and sentence-level interpretations, based on gradient-weighted attention maps derived from all attention layers to track interactions between input features. We show that the proposed model outperforms a model that learns at a segment level ($p$=0.854, $r$=0.947, $F1$=0.947 compared to $p$=0.732, $r$=0.808, $F1$=0.768). For model interpretation, using one true positive sample, we show which sentences within a given speech are most relevant to depression detection; and which text tokens and Mel-spectrogram regions within these sentences are most relevant to depression detection. These interpretations allow clinicians to verify the validity of predictions made by depression detection tools, promoting their clinical implementations.
Artificial Intelligence, speech and language processing approaches to monitoring Alzheimer's Disease: a systematic review
Oct 12, 2020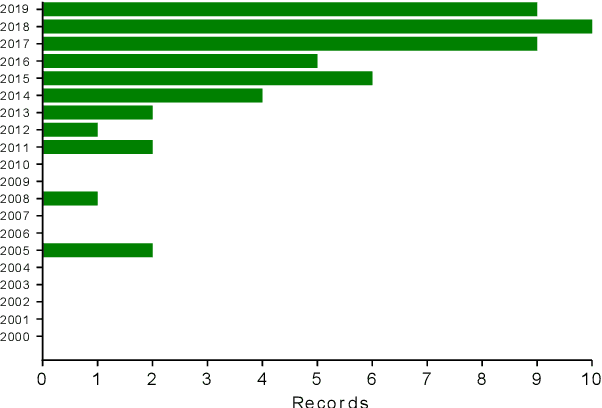



Language is a valuable source of clinical information in Alzheimer's Disease, as it declines concurrently with neurodegeneration. Consequently, speech and language data have been extensively studied in connection with its diagnosis. This paper summarises current findings on the use of artificial intelligence, speech and language processing to predict cognitive decline in the context of Alzheimer's Disease, detailing current research procedures, highlighting their limitations and suggesting strategies to address them. We conducted a systematic review of original research between 2000 and 2019, registered in PROSPERO (reference CRD42018116606). An interdisciplinary search covered six databases on engineering (ACM and IEEE), psychology (PsycINFO), medicine (PubMed and Embase) and Web of Science. Bibliographies of relevant papers were screened until December 2019. From 3,654 search results 51 articles were selected against the eligibility criteria. Four tables summarise their findings: study details (aim, population, interventions, comparisons, methods and outcomes), data details (size, type, modalities, annotation, balance, availability and language of study), methodology (pre-processing, feature generation, machine learning, evaluation and results) and clinical applicability (research implications, clinical potential, risk of bias and strengths/limitations). While promising results are reported across nearly all 51 studies, very few have been implemented in clinical research or practice. We concluded that the main limitations of the field are poor standardisation, limited comparability of results, and a degree of disconnect between study aims and clinical applications. Attempts to close these gaps should support translation of future research into clinical practice.